Download
1 / 47
480 likes | 524 Vues
The Promise of Next Generation Sequencing Junaid Shabbeer, PhD CGMB. Learning Objectives. At the end of this talk you will understand: The principles of NGS The technology behind NGS Applications of NGS in clinical genetics Ethics and issues in the application of NGS. Genetics in Medicine.

E N D
The Promise of Next Generation SequencingJunaid Shabbeer, PhD CGMB
Learning Objectives At the end of this talk you will understand: • The principles of NGS • The technology behind NGS • Applications of NGS in clinical genetics • Ethics and issues in the application of NGS
Genetics in Medicine Understanding genetic variation and its role in disease progression is important in medicine. However studies are challenging, given the size of the genome. Next generation sequencing gives us the power to look deep into the genome.
The Genome is BIG!!! • 3.4 billion bp in 23 chromosome pairs • One cell’s DNA end-to-end stretches 6 feet • All our cells’ DNA would stretch 113 billion miles (to the sun and back 610 times) • Sequence would take 9.5 years to read out loud. • The Human genome sequencing project took 13 years to complete at a cost of $2.7 billion • NGS cuts the time & cost to sequence the genome
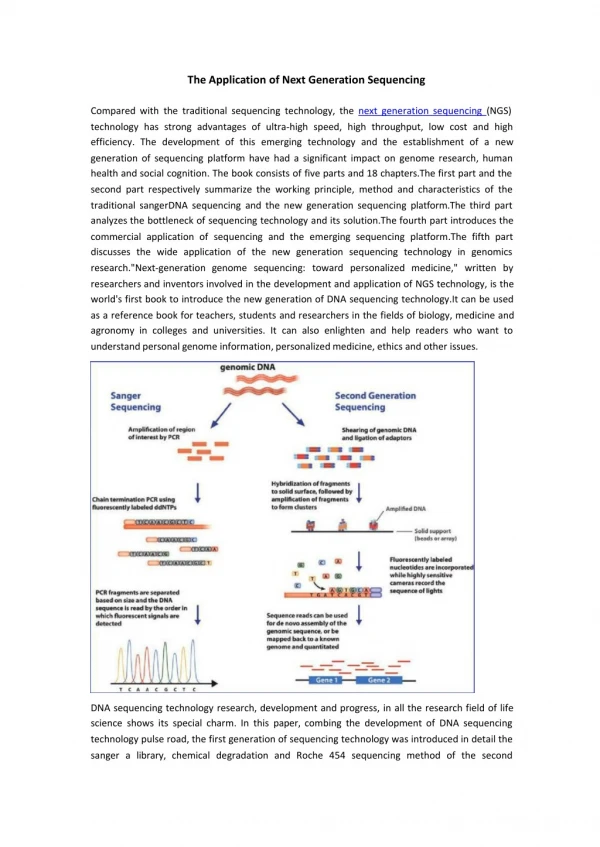
The Classical Way of Sequencing Chromosome Genetic Map Physical Map Large Clones Physical Map Small Clones DNA Sequence A A C G T C A G G C C T C A G
DNASequencing Aim: Find the sequence of A, C, G, T in DNA Method: Isolate genomic DNA Amplify template (DNA target) Incorporate chemically modified bases into physical sequence- Make new strands with modified bases (Chain termination/Sanger dideoxy method) Read bases
Challenges Met by NGS • Need for speed and lower costs. • There is no machine that takes long DNA as an input, and gives the complete sequence as output. • Can only sequence ~500 letters at a time by conventional sequencing.
Next Generation Sequencing • Breaks all physical constraints that limit conventional sequencing: • No need for libraries (still need to amplify) • Microfluidics breaks volume constraints • No need for physical separation of fragments • Bioinformatic tools enable big data analysis • Faster and Cheaper
Steps in Next Gen Seq • Immobilize DNA fragments to solid surface (chip, bead, flow cell). • Amplify/enrich each template molecule. • Sequence each molecule in emulsion, detecting signal base by base. • Software aligns reads to a reference sequence.
Illumina Sequencing • Templates immobilized on flow cell surface. • Solid-phase amplification of each template molecule. • Avg of 1000 copies/molecule in a cluster. • Up to 10,000,000 single molecule clusters per cm2 • Single base by base calls made from signal intensity measurements during multiple strand synthesis cycles.
Bases are incorporated one at a time and their signal captured to build a sequence.
Sequence Analysis • Sequencing and genome assembly • Alignment to reference genome • Identification of variations • Map variations to find those with functional significance
NGS in Personalized Medicine • Screening individual genomes to identify genetic variants that: • cause disease • predispose to disease • determine drug response • Both prenatal and adult screening possible.
Challenge to Clinical Use The genome is still big!
How to ID Harmful Variants? No Disease Hemophilia = Variation in DNA that causes harmful change
Childhood Disease Screening by WGS Disease gene identification in newborns can lead to targeted treatment before organ damage occurs.
The Challenge & Need of Finding Childhood Monogenic Disease Genes • There are 3,517 diseases with a known causative gene that affect 4% of children • 4.1 million babies born in the US/year • 30% with congenital findings • 1 in 20 admitted to NICU
Results of WGS:Challenge & Opportunity • In a typical genome, there are: • ~ 4 million nuclear variants/genome • ~ 10, 000 gene associated variants • ~ 2,000 <1% allele frequency • ~ 900 associated with disease causative genes
Which Gene(s) is the Culprit? The Children’s Mercy Hospital approach: • Symptom and sign assisted genome analysis. • Map clinical features to genetic diseases. • Target genes to sequence in families.
Solutions to Finding the Gene of Interest • Sequence genomes of family members • Sequence the exome • Sequence the transcriptome • Use gene panels, eg CVD Panel • Couple with targeted analysis based on clinical and biochemical information
Finding Disease-Linked Genes Disease Present Disease gene Disease Absent Variant
Case Study 1 Using WGS to Identify Familial Disease-causing Gene Variants
WGS Case Presentation • Male twins diagnosed cerebral palsy age 2. • Age 4 symptoms worsen (involuntary muscle spasms) • Rediagnosed with dopa-responsive dystonia age 6; respond well to L-dopa treatment (substitutes for missing dopamine). • Age 7 severe breathing problems develop.
Strategy • Sequence family’s genomes to find causative mutation for better diagnosis to guide more effective therapy • Whole genomes sequenced:
WGS Findings • Mutations found in three possible causative genes. • Two genes had no known purpose. • Suspect mutations found in gene for SPR (sepiapterin reductase) • SPR associated with dopa responsive dystonia. • Twins had two mutated copies of SPR; one from the mother, one from the father.
The Benefit • Mutant SPR disrupts dopamine AND serotonin production. • Both critical neurotransmitters. • Therefore, dopa treatment alone not sufficient; need to substitute for both neurotransmitters. • When 5-HTP added to therapy, twins’ symptoms improved dramatically.
Case Study 2 Using Exomic Sequencing to Identify Novel Gene Variants causing Specific Disease Phenotypes
Whole Exome Sequencing Exome sequencing used to identify novel gene variants associated with familial pulmonary arterial hypertension
The PAH Problem • PAH is a rare, progressive and fatal disorder that causes reduced blood flow from heart to lungs. • Several genes linked to 75% of cases. • 25% cases of unknown etiology.
Finding the Answer with Whole Exome Sequencing • Samples collected from three affected members of one family with no known mutations. • Whole exome sequencing performed on all samples. • Filtered out common variants. • Ignore variants that did not adhere to AD mode of inheritance suggested by pedigree study. • Reject variants with benign effects.
What Whole Exome Sequencing Found • 19 SNPs and 5 indels of potential significance found. • Focus on one SNP in KCNK3. • Gene encodes part of K channel involved in resting membrane potential & pulmonary vascular tone. • SNP associated with disease in one family. • Multiple KCNK3 variants subsequently discovered in other affected families. • Electrophysiological studies show mutations lead to loss of channel function.
Benefit to PAH Patients • More rapid and definitive diagnosis. • Drug can rescue some mutations in cell cultures. • Phospholipase inhibitor increases density of some mutant channels to non-mutant levels. • Potential therapeutic for some PAH patients.
Genomic Sequencing Makes DNA Hunting Easier • Massive parallel sequence reads. • Deep sampling and uniform coverage generates consensus sequence. • Instruments allow better detection. • Statistical tools allow handling of big data. • Allows for detection of rare or low copies.
Other Clinical Applications of NGS • Infectious disease testing • Cancer diagnostics • Prenatal diagnostics
In Oncology • Sanger-led team cataloged mutational signatures in 30 top cancer types. • 7,000 cancer genomes sequenced to unravel mutation profiles in the 30 cancer types. • Found 20 mutational signatures in distinct combinations in tumors depending on the patient's age, cancer type, past exposures to DNA mutating agents, etc.
Non-invasive Prenatal Screening for T21 • Cell-free DNA (cfDNA) is short DNA fragment (50-300 base pairs) • In pregnancy, cfDNA from both the mom and fetus are in maternal blood • cf DNA can be isolated and sequenced on an NGS platform
cfDNA testing for T21 Extra fragments derived from fetal T21 Fetal cfDNA • Each bar represents thousands of cfDNA fragments. The over-abundance of T21 fragments can be detected by sequencing. Maternal cfDNA Reference chromosome Chromosome 21 fragments
Ethics & Issues • Unintended discovery (incidental findings) • Right to pick and choose sequences? • Who gets and interprets results? • Do we know what it all means? • Privacy concerns • Patents • Rights of the unborn
The Future • Expanded use of WGS in diagnostics • Improved prognostics and therapeutic decision making • More non-invasive prenatal Dx • Cost reductions; $1000 genome?