Download
1 / 44
450 likes | 694 Vues
Outpatient care in the era of MRSA. Julie Gutman, MD Pediatric Infectious Disease Fellow August 29, 2007. MRSA. Basic Micro History of MRSA emergence Genetic markers Resistance testing Treatment Eradication. Staphylococci. Gram-positive Facultative anaerobes Grow in clusters

E N D
Outpatient care in the era ofMRSA Julie Gutman, MD Pediatric Infectious Disease Fellow August 29, 2007
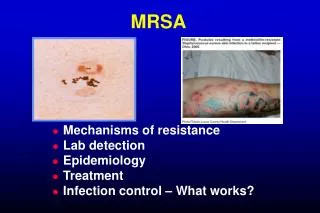
MRSA • Basic Micro • History of MRSA emergence • Genetic markers • Resistance testing • Treatment • Eradication
Staphylococci • Gram-positive • Facultative anaerobes • Grow in clusters • Strep usually grow in chains • Catalase test(+) • distinguishes from strep spp. which are (-) • S. aureus & S. epidermidis are most important clinically
Emergence of MRSA • First described in 1960 • One year after introduction of methicillin! • Initially most cases were “hospital acquired” • Risk factors for Hospital Acquired: • Hospitalization, Surgery, Dialysis • Permanent indwelling device • Trach, G-tube, foley, CVL
Evidence of MRSA in the Community • 3% colonized with MRSA at center X • 24% colonized with MRSA at center Y JID, Volume 178 (2), August 1998
Increasing incidence of CA- MRSA in Hospitalized Children • Retrospective review: Compared August- July of 1988-1990 and 1993-1995 • CA-MRSA disease increased: • 8 in 1988-90 to 35 in 1993-95. • 10/100,000 to 259/100,000 (P<.001) • Noted a difference in susceptibility of isolates from children with risk factors for MRSA vs. those with no risk factors Herold et al. JAMA. 1998;279:593-598
MMWRFour Pediatric Deaths from CA-MRSA- Minnesota and North Dakota, 1997-1999 • First report of fatal outcomes associated with MRSA • Type MW2 (USA400) Methicillin-resistant Staphylococcus aureus (MRSA) is an emerging community-acquired pathogen among patients without established risk factors for MRSA infection This report describes four fatal cases among children with community-acquired MRSA; the MRSA strains isolated from these patients appear to be different from typical nosocomial MRSA strains in antimicrobial susceptibility patterns and pulsed-field gel electrophoresis (PFGE) characteristics. MMWR, August 20, 1999 / 48(32);707-710
Incidence of CA-MRSA Disease Fridkin, et al. NEJM 2005. 352: 1436-44.
Sequencing of CA-MRSA (MW2) • Identified SCCmec IV with mecA gene • Lacked the multiple resistance genes found in HA-MRSA (SCCmec II, also I and III) • Homology with HA-MRSA genome ~ 95% • homology is 99.7% between HA-MRSA strains • 18 new virulence factors • Rapid growth rate- survival advantage • doubling time 13-23.5m VS. 34.8 and 46.8m for HA-MRSA Baba, et al. 2002. Lancet. 359:1819
MRSA Genetics- SCCmecIV • Staphylococcal cassette chromosome (SCCmec) – mobile genetic element • Methicillin resistance mecA gene • Produces altered penicillin binding protein PBP2a • CA-MRSA generally SCCmec IV • smaller & more mobile than other SCCmec • HA-MRSA carries type II • predominant circulating clones • USA300 and USA400
Staphylococcal Cassette Chromosomes (SCC-mec).Okuma, JCM 2002
MRSA Strain Typing • Pulsed-field gel electrophoresis (PFGE) • Uses Sma1 restriction endonuclease • Clones USA100- USA1000 have been designated • Clones USA300 and USA400 predominate • PCR-based methods • spa typing • DNA-sequencing of repeat regions of the Staphylococcus protein A gene (spa): repeats are assigned a numerical code and the spa-type is deduced from the order of specific repeats • multilocus sequence typing (MLST) • Uses the sequences of 7 house-keeping genes and assigns an allelic type to each sequence.
Naima, et al. JAMA 2003 Antimicrobial SusceptibilityCA-MRSA vs HA-MRSA
2006 Wounds • ECH • MRSA [65% incidence {all sources,locations}] • S.aureus • Anaerobes • E.coli • Streptococcus pyogenes (gpA strep) • Pen 100% S, Erythro 93.1% S, Clinda 99.5% (CID.05. 41:599) • Enterococcus faecalis • Ceph’s are ineffective • “SPICE” and “M” • Serratia, Providencia, Indole + Proteus, Citrobacter, Enterobacter and Morganella Source: Misys Incidence query Courtesy of Dr. Jerris
2006 AntibiogramEgleston • Single isolate per patient per year Clinda TMP/SMX Cipro
Inducible Clinda Resistance • Mediated through erm gene – MLSB • Alteration in the 23S ribosomal RNA • Part of 50S ribosomal subunit • Occurs through methylation of adenine • Confers resistance to: • erythromycin and most other macrolides (M) • lincosamides (L, lincomycin, and clindamycin) • streptogramin type B (SB). Consider in all Erythro Resistant isolates!!!
D- test for inducible clindamycin resistance • NO induction • msrA-mediated erythromycin resistance • Erythro – R • Clinda – S Negative reaction Courtesy of Dr. Jerris
D- test for inducible clindamycin resistance • Inducible • clindamycin resistance • (erm-mediated) • Erythro – R • Clinda – R 15 - 26 mm Positive reaction Photos courtesy of J. Jorgensen and K. Fiebelkorn. Courtesy of Dr. Jerris
EglestonInducible Clinda Resistance ‘06 *Note that the rates vary dramatically depending on the site and patient population Courtesy of Dr. Jerris
Skin and Soft Tissue Infections • CHOA - 2006 • WOUNDS: • 288 isolates with MRSA (1 isolate per patient per year) Erythro Resistant and Clinda Susceptible ► 6/288 were D-zone test positive (2.1%) - Outpt. 2/186 (1%) - Inpat. 4/102 (4%) • @30% of population carry this organism-CDC Courtesy of Dr. Jerris
Syringes FOR QUALITY RESULTS, SEND TISSUE, FLUIDS ,OR ASPIRATES (SAME SPECIMEN FOR PATHOLOGY BUT NOT IN FORMALIN) Courtesy of Dr. Jerris
Vancomycin Intermediate(resistant) S. aureus (VISA) • Japan, 1996: first documented case of VISA • MIC=8 ug/mL • US, July 1997, VISA-associated peritonitis • isolate was susceptible to rifampin, chloramphenicol, bactrim, and tetracycline. • National Committee for Clinical Laboratory Standards breakpoints for susceptibility: • susceptible ≤4 ug/mL • Intermediate = 8-16 ug/mL • resistant ≥32 ug/mL MMWR, August 22, 1997; 46(33);765-766
Spectrum of Disease • more virulent than HA-MRSA. • Infection of skin or soft tissue • Osteomyelitis • Pyomyositis • Necrotizing pneumonia • Severe sepsis • purpura fulminans, DIC, and bilateral adrenal hemorrhage • Necrotizing fasciitis • Thromboemboli
Panton Valentine Leukocidin (PVL) • Bicomponent, pore-forming leukotoxin • LukS-PV and LukF-PV • Produces lysis of PMNs • Carried on an integrated bacteriophage (phiSLT) • Causes dermonecrosis if injected into skin of animals • Associated with severe disease in CA-MSSA and CA-MRSA • More frequently associated with sepsis, high fever, leukopenia, hemoptysis, pleural effusion and death than PVL (-)
Panton Valentine Leukocidin (PVL) BUT • PVL-negative (lukS/F-PV knockout) strains of USA300 and USA400 were as lethal as wild-type strains in a mouse sepsis model, and they caused comparable skin disease
Outpatient Management of CA-MRSA + Assumes >90% “D” test negative, erythro resistant CA-MRSA Baker, AAP News September 2004
For life threatening disease • Nafcillin + Vancomycin + Clinda (effect on toxin) + Gent or Rifampin • +/- Ceftriaxone for gram negatives • NO good data to support this combo!
A Note about Wounds… • For abscesses, DRAINAGE is key! • Abscesses<5 cm – I&D alone sufficient!
Antibiotic Choices for Staph • Nafcillin- preferred treatment for MSSA! • More rapid clearance of blood cultures than Vanc • Bactrim- some proven efficacy for SSI • Does NOT cover strep! • Clindamycin- covers strep and staph! • 10-20% resistance, should NOT use as monotx for severe infections! • Vancomyin- DOC for MRSA
Antibiotic Choices for Staph • Gentamicin- used a an adjuntive therapy- synergistic activity with Vanc • Rifampin- proven efficacy in setting of prosthetic valve endocarditis, otherwise, little data • Should never be used as monotherapy for treatment!
New Antibiotic Choices for Staph • Linezolid • Skin and soft tissue infections, pneumonia • Have been reports of failure when used for endocarditis • Can be given PO • SE: thrombocytopenia, optic neuritis, peripheral neuropathy • Daptomycin • Skin and soft tissue infections, bacteremia, endocarditis with MRSA • NOT for pneumonia! • SE- musculoskeletal. Monitor CPK.
Others you may hear about… • Tigecycline- approved for MRSA skin ond soft tissue infections • Extremely broad spectrum!! Covers VRE, complicated intra-abdominal infections • SE: GI- Nausea, Vomiting • Quinupristin-Dalfopristin- approved for VRE, MSSA, not MRSA • Requires central line • Severe myalgias, arthralgias • Dalbavancin- once weekly dosing • Not yet FDA approved!
Prevention Strategies, MMWR Feb 7,2003 / 52 (05);88 Community setting: • Thoroughly clean towels, bed linens, personal clothing •Thoroughly wash cuts and abrasions with soap and water •Disinfect athletic equipment, benches, personal equipment with commercial disinfectant or diluted bleach ( 1 tablespoon bleach in 1 quart water) •Common sense personal hygiene Individual patients: • Local treatment I & D (antimicrobics) Courtesy of Dr. Jerris
Decolonization- Cochrane Review 6 trials (384 participants)
Decolonization- Cochrane Review • SE in up to 20% of systemic agent use. • All trials reported development of resistance • Authors' conclusions • Insufficient evidence to support use of topical or systemic antimicrobial therapy for eradicating MRSA. • Need for large RCT!
Decolonization 2% chlorhexidine gluconate wash + 2% mupirocin intranasally + Oral Rifampin + Doxy for 7 days • 74% of treated vs. 32% untreated had negative cultures at 3 months Simor et al., CID 2007. 178:44.
Our Protocol • Clinda or Bactrim + Rifampin PO • Mupirocin daily x 7 d to nares of ENTIRE FAMILY • Chlorhexidine gluconate washes daily for a week, then 1-2 times weekly • (can substitute bleach baths) • Cross your fingers and pray.
Blood Culture VOLUME • Volume of blood drawn for culture is the MOST IMPORTANT variable in detecting bacteremia or fungemia • MAX volume per BC System For adult patients, the yield of pathogens increases in direct proportion to the volume of blood that is cultured from 2 to 30 mL. The yield still increases when 40 mL (or even higher) volumes of blood are cultured, although the increase may no longer be in direct proportion to the volume of blood cultured. For pediatric patients, the limited data that has been published also indicate that the yield of pathogens increases in direct proportion to the volume of blood that is cultured [Li J, Plorde J, and Carlson L. 1994. Effects of volume and periodicity on blood cultures. J Clin Microbiol. 32:2829-2831] Courtesy of Dr. Jerris
4 pandemic MRSA clones derive from 2 distinct backgrounds Oliveira, Lancet 2002