Download
1 / 14
160 likes | 265 Vues
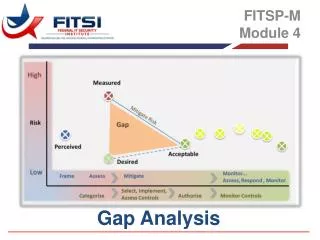
GAP ANALYSIS REPORT tuberculosis component September 2011. INTRODUCTION.

E N D
INTRODUCTION • The Ministry of Health and Social Welfare (MOHSW) through the National TB/Leprosy Programme (NTLP) in collaboration with Programme for Appropriate Technology in Heath (PATH) commissioned a consultant – Prof G. B. Milgiori and Mr. Alberto Matteelli Giusto of WHO Collaborating Centre, Tradate Varese Italy • Other partners involved were Medical Sciences for Health (MSH) • The Gap Analysis was conducted from 4 – 8 July, 2011 in 3 Municipalities in Dar es Salaam and Partners Supporting TB and TB/HIV control in the country • Dissemination of findings was done on 11th July, 2011 at Courtyard Hotel and was attended by more than 30 stakeholders and partners. The list of attendants is available • Comments from the dissemination meeting were incorporated into the final report. • This dissemination is intended to inform TNCM members of the TB gaps highlighted by the GAP analysis and seek directives on how to resolve them
MAJOR GAPS IDENTIFIED • Outstanding TRP comments from Round 9 not completely addressed, in particular: • coordination between partners • lab platform to support MDR-TB • Quality of patient data as raised by the Local Funding Agent • Inadequate transparency in funds from other donors and partners • Low absorption capacity based on slow spending in phase 1 • Budgetary issues • incorrectly classification of cost categories • High unit costs for pharmaceuticals and equipment • Use of lump sums instead of separate costs for each item • Unclear rate of inflation applied • Performance Framework - Outcome indicators not always clear
Gap 2 • The TRP is concerned that the issue of poor quality of data (raised by the Local Funding Agent (LFA) audit December 2009: C rating) is not adequately addressed. • Solutions: Describe in details recording and reporting system and data flow and quality to ensure procedures in details with NTLP and LFA
GAP 3 - Funding • Difficult to assess trends in partners funding. Aggregation of US govt support with other sources (German Leprosy Relief Association (GLRA), World Health Organization (WHO), Global Development Finance (GDF) and World Bank not enough • Solution1: NTLP to describe who is funding what, the disaggregated support by US Gov, GLRA, WHO, GDF, WB & UNITAID as preliminary step of the writing process, following ICC meeting with partners. • Solution2: NTP needs to quantify the amount allocated for TB laboratories within the WB proposal for Tanzania.
Gap 4 • In view of the delay in signing the Round 6 Phase II grant and slow spending in Phase I, the TRP is concerned about absorption capacity. • Solution 1: NTLP to describe the process, difficulties encountered and remedial actions undertaken. • Solution 2: Describe role of the focal person(s) recruited by MoHSW to coordinate GF implementation (disbursements, technical and financial reporting) and any other GF obligations needs to be emphasized.
GAP 5 BUDGET - 1 • Many items are incorrectly classified per cost category hindering appropriate assessment (e.g. no Procurement and Supply Management cost has been documented) and Many unit costs for pharmaceuticals and equipment are set substantially higher than international standards • Solutions: .NTLP to identify the items concerned and capture it in R11 proposal with consultants’ support and overall input by SMH • Solutions: NTP to identify the items concerned and capture correct costs it in R11 proposal with consultants and MSH support
GAP 5 BUDGET -2 • Use of Lump sums are given for several items (e.g. Reagents (various) at US$ 200,000). • Unclear rate of inflation applied, at times 6 percent per year and not adjusted to Forex variations • Solutions: NTP to identify the items concerned and capture correct quantification/costs in R11 proposal with consultant and MSH support • NTP to apply the correct inflation adjusted for Forex variations quantification in R11
GAP 6 • No evidence that current incentives are provided under the framework of a health sector agreed policy. • Solutions: NTP to seek an approved policy letter signed by Permanent Secretary demonstrating the Country’s policy
GAP 7: PERFORMANCE FRAMEWORK: • Indicators to output of activities that do not really reflect the performance of the program in terms of coverage of target groups and quality of services provided should be removed from the performance framework. • Include lab performances (EQA AFB, validation of DST 1st and 2nd line) • Include outcomes for MDR
GAP 8. TB/HIV COLLABORATIVE ACTIVITIES • No clear strategy is described for integration of tuberculosis control activities in work place already addressing HIV related activities • Solutions: Revise TB/HIV components of the proposal to incorporatespecific interventions to cover workplace TB/HIV issues
THEMATIC AREAS FOR GFR11 • Goal: To reduce the morbidity and mortality of Tuberculosis by 25% by 2015 compared to 2009. • Objective 1. Pursue high quality DOTS expansion and enhancement • SDA 1.1: Attain political commitment with adequate and sustained financing for TB • SDA 1.2: Improve diagnosis of TB through quality assured bacteriology • SDA 1.3: Procurement and supply management of first line drugs • SDA 1.4 Monitoring and evaluation and impact measurement • SDA 1.5 Management, coordination and supervision • SDA 1.6 Human resource development
THEMATIC AREAS .. CONT .. • Objective 2. Address TB/HIV activities, MDR-TB and other challenges • SDA 2.1 TB/HIV • SDA 2.2 MDR-TB • SDA 2.3 High risk groups • SDA 2.3.1 Addressing prisoners, TB contacts • SDA 2.3.2 Infection control • SDA 2.3.3 Childhood TB
THEMATIC AREAS … CONT .. • Objective 3. Contribute to health system strengthening • SDA 3.1 Practical Approach to Lung Health (PAL) • Objective 4. Engage all care providers in TB control • Objective 5. Empower people with TB and communities • SDA 5.1 Advocacy, Communication and Social Mobilization • SDA 5.2 Community TB care • Objective 6. Enable and promote operational research • SDA 6.1 Program-based operational research