Download
1 / 21
220 likes | 516 Vues
Enhanced Recovery Processes. Ron Collins, MD FRCP(C) Clinical Assistant Professor, APT, University of British Columbia Medical Director, Surgical Services Project Lead, Enhanced Recovery Interior Health Authority Staff Anesthesiologist, KGH. Disclaimer.

E N D
Enhanced Recovery Processes Ron Collins, MD FRCP(C) Clinical Assistant Professor, APT, University of British Columbia Medical Director, Surgical Services Project Lead, Enhanced Recovery Interior Health Authority Staff Anesthesiologist, KGH
Disclaimer • Member of Advisory Panel to Fresenius-Kabi (FLOW: Fluidop.com) • None of the content or ideas relate to papers from Dr. Joachim Boldt
Enhanced Recovery After Surgery “The profession has place high value on developing the basic science of medicine: it has not emphasised the process by which the science is translated into practice…” Eddy, DM. N Engl J Med 1982;307:343-7
Enhanced Recovery Is…. • Evidence-based clinical pathways • Multidisciplinary in scope • Outcome driven • Better for patients • Better for healthcare organizations • “Complex” task to implement • Up to 20 elements or milestones
Relative Contributions to Adverse Events and Excess Length of Stayadapted from Fry et al, J Am CollSurg 2008;207:698-704
“Ultimately, improving quality will require efforts that go beyond outcomes assessment alone. Future work should aim to improve our current understanding of processes of care associated with superior surgical outcomes.”Fry et al., J. Am CollSurg 2008;207:698-704
Enhanced Recovery After Colorectal Surgery • Evidence-Based Surgical Care and the Evolution of Fast-Track Surgery • Kehlet, H. and Wilmore, D.; Ann Surg 2008;248:189-98 • Consensus Review of Optimal Peri-operative Care in Colorectal Surgery • ERAS Group; Arch Surg. 2009;144(10):961-969
Colorectal Clinical Pathway • Discreet steps • Evidence-Based • Pre-operative • Intra-operative • Post-operative • Challenges traditional processes
Pre-Operative Elements • Overview of pathway • Establish expectations • No mechanical bowel preparation • Carbohydrate beverage (2 ½ hrs) • No sedative premedication
Intra-Operative Elements • TEA T9 or T10 • Narcotic sparing anesthetic • Goal Directed Fluids with CardioQ • Active warming • Routine anti-emetics • No NGs, no drains
Post-Operative Elements: PAR • Optimize epidural analgesia • Narcotic sparing • High-flow O2 for 1 hour • May chew gum in PAR • Full fluids in PAR
Post-Operative Elements: Surgical Ward • Full fluids Day 0, DAT Day 1 • Out of bed 6 hours Day 1 • Activity specified • May chew gum in PAR • Full fluids in PAR
ROI Methodology Reaction Learning Application Business Impact ROI Intangible Measures Specific Measureable Actionable Realistic Timeframe
ROI Methodology • ERACS evaluation based on first 16 pts. • Interviews with 5 individuals • Surveys from 33 individuals • KGH records • ERACS records • CIHI data for RIW • Cost estimates for ERACS start-up
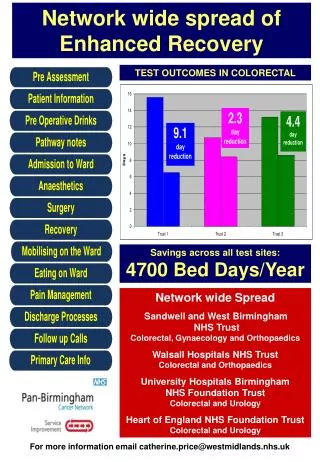
Enhanced Recovery After Colorectal Surgery 88% of staff feel ERACS is vital to the success of IH. 87% of staff feel that ERACS provides better patient care. Opportunities to improve infrastructure and demonstrate adaptability. “The ERACS process is better for patients, and that is what my life’s work is about.” Surgical Ward Nurse
ROI Methodology • Return on Investment: • ERACS Cost Summary: $56,413.45 • ($21,500 for ROI) • Mostly one time costs • Traditional cost (RIW 3.42): $15,884.81 • ERACS cost (RIW 1.76): $8,194.42 • Savings: $7,690.39 ($123,046.24)
Enhanced Recovery After Colorectal Surgery Length of stay reduced from 12.8 to 4.0 days. RIW reduced from 3.41 to 1.76 Benefit/cost ratio: 2.18 ROI: 118% CIHI estimated cost reduction of 48.4%.
How do you measure success? • CIHI assigned RIW decreased • >90% of colorectal patients enrolled • Fewer complications overall • Fewer complications in high-risk groups • Caregiver satisfaction • This is the ‘new normal’ • There are opportunities….. • Requests from additional surgical groups!