Download
1 / 23
230 likes | 343 Vues
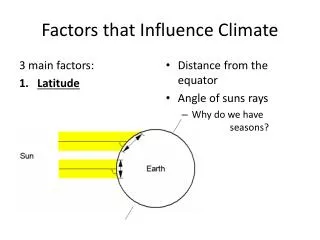
Factors that Influence Utilization of Low Cost Dental Resources for Children. Student Name University of California, Irvine Field Studies, Spring 2008. General Background. Tooth decay (TD): Most common chronic problem for children in US Number one health problem for children in California.

E N D
Factors that Influence Utilization of Low Cost Dental Resources for Children Student Name University of California, Irvine Field Studies, Spring 2008
General Background • Tooth decay (TD): • Most common chronic problem for children in US • Number one health problem for children in California *21,000 children surveyed Dental Health Foundation, 2006
General Background • Tooth decay- easily preventable, but a progressive infection if left untreated • Consequences of untreated TD: • Chronic Pain • Low self-esteem • Poor Nutrition • Tooth loss • Sleep deprivation
Key Terms • Dental resources • Caregivers • Provider • School Health Curriculum • Medicaid & Denti-Cal • Beneficiary
General BackgroundPopulation at Risk: Low-income children Latino children • 72% of Latino children have a history of TD • 30% need treatment • 26% had rampant decay • Nearly twice the rate of non-Latino white children surveyed • 1/3 of low income children have untreated TD vs. the 1/5 of higher income children • 40% of children w/ no insurance vs. 21% children w/ private insurance Dental Health Foundation, 2006
What are the Problems? • California ‘s reimbursement rate for publicly funded dental care are among the lowest in the nation • Less than half of dentists accept Denti-Cal patients • Low service use for those that qualify for Denti-Cal California HealthCare Foundation, 2007
Purpose of the Study • To investigate the dental resources, particularly those promoted through the elementary schools, available in a community in which low-income families are the minority • To investigate factors that influence caregivers to use or not use these dental resources.
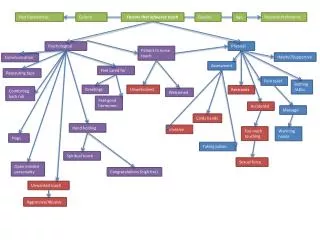
Theory of Planned Behavior Subjective Norm Attitude Behavior: Utilizing Dental Resources Intention Perceived Behavioral Control Ajzen, 1991
Review of Literature Attitude Mother Dental Phobia: • Caregivers reported dental care experiences influenced their dental beliefs and behaviors, (Kelly, Binkley, Neace& Gale, 2005, Milgrom, Mancl, King, Weinstein, Wells & Jeffcott, 1998). Child Dental Phobia: • Caregivers were less likely to have taken their child to the dental office if their child expressed fear of the dentist, (Milgrom, Mancl, King, Weinstein, Wells & Jeffcott, 1998). Education Level: • Different levels of education attainment influence reasons caregivers took the child to the dental office, (Kelly, Binkley, Neace& Gale, 2005).
Review of Literature Subjective Norm • School Health Curriculum: Child health curriculums with a parent component are more effective for the child and can also benefit the parent, (Gray, Byrd, Crossman, Chromiak, Cheek, & Jackson, 2007, Hopper, Munoz, Gruber & Nguyen, 2005). • Government & Nonprofit dental referrals: Children in the WIC program are more likely to use preventive and restorative services and are less likely to use emergency services than WIC nonparticipants, (Lee, Gary Rozier, Norton, Kotch & Vann Jr., 2004).
Review of Literature Perceived Behavioral Control (PBC): • Socioeconomic Status (SES)Low SES families experience competing needs, such as other health issues, inflexible work hours, and distance to providers, which drain already limited resources available for dental care. (Frazier, Jenny, Bagramain, Robinson &Proshek, 1977) • The Role of the Provider Medicaid patients face lack of providers and have trouble scheduling appointments at offices that do accept Medicaid (Mofidi, Rozier& King, 2002) Providers appear to hold condemnatory attitudes toward lower class clients. (Frazier, Jenny, Bagramain, Robinson &Proshek, 1977)
Research Questions 1. What types of dental resources are offered in communities in which low-income families are the minority? 2. What factors influence low-income families to utilize or not utilize these dental resources?
Methodology: Research Design • Mixed Methods Study: • Site interaction • Observe participant interaction with health curriculum • Informal and formal interviews with key informants • Survey with an open-ended comments section at the end • Triangulation: • Multiple site observations • Multiple informant interviews • Site Selection: • Guidance Resources, Irvine Unified School District • Selection based on involvement with health curriculum
Methodology: Participants • Participants knowledgeable about the educational resources: • 6 classes observed: • 2 kindergarten classes & 4 first grade classes • About 19-23 students in each class • 4 Teachers interviewed: • 1 teacher piloted the program & taught 3 yrs • 3 teachers taught the program for 3 yrs • 1 Nurse interviewed: • Piloted the program • Gives lessons during the GBS
Methodology: Participants • Participants knowledgeable about community dental resources: • 3 Nurses and 1 health clerk interviewed: • All had 2+ years with the district • 2 participated at the 2007 free dental health screening • 1 involved in School Readiness program • 1 Community Dentist interviewed: • Has experience with Denti-cal and pediatric dentistry in the Irvine Community
Methodology: Data Analysis • Extensive review of field notes, RQ’s and theoretical framework • Peer review and evaluation of preliminary findings • Coding, sorting, and recording • Hi-lighting, boxing, underlining, and symbols • Identifying common themes and co-occuring patterns • Tallying and Matrix Enumeration used during classroom observations
Theory of Planned Behavior, revisited Attitude Subjective Norm Behavior: Utilizing Dental Resources Intention Perceived Behavioral Control Ajzen, 1991
Findings: Subjective Norm • State Requirements • Free Dental Health Screenings • School Policies Program • “There’s so much going home that we try keeping it in the classroom as much as we can. Student issues are sent home …How many of them get home, I don’t know.” -Mrs. Alison • “I saw only one issue… about puberty and personal hygiene. We had a really interesting discussion about it ….” • Nurse referral • “I don’t see that many students come in with tooth aches during the year, but when they do I take it seriously, and call home.” –Nurse Bev
Findings: Perceived Behavioral Control • Difficulty in Finding a Provider • “Medi-cal providing is hard in this district and town, because there aren’t that many. “Medi-cal only pays a certain amount of money, so dentists and physician say I will take so many Medi-cal patients….” –Nurse Linda • Resident & Coverage Status • “But we have a huge influx of families out of the country, and so they need help a little bit, because they don’t know where to go” -Nurse Bev • “New to the area”, have used them in other areas and want to know what’s available here to use. They’ve been in the system before” –Nurse Reyna
Discussion • Attitude: • Caregiver and child dental phobia: not observed • Education level: confirmed • Subjective Norm: • School health curriculum: confirmed • Government and nonprofit dental referral: confirmed • Perceived Behavioral Control: • SES: not observed • The role of the provider: confirmed
Limitations Educational Resources Community Resources • Data collection could not be from direct contact with parents • Did not consistently observe dental lessons • Did not have consecutive observations with the same class of participants • Informant knowledge was limited about parent attitudes and utilization of program • Data collection could not be from direct contact with parents • Dentist was not a Denti-cal provider in the Irvine Community • Informants were only able to provide general comments on parent attitude and utilization of resources
Implications • To Practice • Proactively target low-income families through the Irvine Support to Families in Need Task Force • Strengthen GBS parent component • To Research • Need further research involving direct observation and interview with parents • A follow up research study that can show the effect of: • The growing low income population • Program implementation
Acknowledgements Dr. Castellanos Debra Bianchi Kim Snodgrass Nancy Colocino Teri Skinker The Class