Download
1 / 39
390 likes | 540 Vues
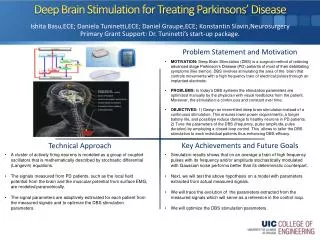
Management of Moderate to Severe Parkinson’s Disease. Benjamin L. Walter M.D. Medical Director, Deep Brain Stimulation Program Neurological Institute University Hospitals Case Medical Center. What is Parkinson’s disease?. Not all that look like Parkinson’s is Parkinson’s.

E N D
Management of Moderate to Severe Parkinson’s Disease Benjamin L. Walter M.D. Medical Director, Deep Brain Stimulation Program Neurological Institute University Hospitals Case Medical Center
What is Parkinson’s disease? University Hospitals Neurological Institute
Not all that look like Parkinson’s is Parkinson’s • Idiopathic Parkinson’s disease = “typical Parkinson's disease” • Secondary Parkinsonism • Parkinson’s Plus = parkinsonism + … some other features • PSP (Progressive Supranuclear Palsy) • MSA (Multiple Systems Atrophy) • DLB (Diffuse Lewy Body Disease) University Hospitals Neurological Institute
The symptoms of Parkinson’s Disease vary from patient to patient • Must have2of the following: • Stiffness • Tremor at rest • Slowness • Postural Changes or Gait Changes (for example, shuffling or freezing) • And should be responsive to dopamine medications University Hospitals Neurological Institute
Parkinson’s disease is relatively common • 2nd most common neurodegenerative disease • 1/500 live with Parkinson’s disease • Over the age of 60, 1/100 people have PD • May be more common in men University Hospitals Neurological Institute
People with Parkinson’s are like snowflakes University Hospitals Neurological Institute
Tests for Parkinson’s Disease • Genetic tests for only 10% of patients • MRI, CT scans—do not make diagnosis • When suspicion of another cause other laboratory tests may be ordered • The best test is the expert clinical examination by a movement disorders specialist University Hospitals Neurological Institute
Lewy bodies form in the brain University Hospitals Neurological Institute
Progression of Pathology in PD Braak H, Del Tredici K, Bratzke H, et al: Staging of the intracerebral inclusion body pathology associated with idiopathic Parkinson's disease (preclinical and clinical stages). J Neurol 249 Suppl 3:III/1-5, 2002 University Hospitals Neurological Institute
Levodopa Compounds Carbidopa/levodopa (Sinemet) Controlled Release Carbidopa/levodopa (Sinemet CR) Carbidopa/levodopa/ entacapone (Stalevo) Dopamine Agonists Pramipexole (Mirapex) Ropinerole (Requip) Pergolide (Permax) Apomorpine (Apokyn) Rotigitine (Neupro) Patch Anticholinergics Trihexaphenedyl (Artane) Benztropine (Cogentin) Parsitan Kemadrin NMDA Antagonists Amantadine (Symmetrel) MAOB Inhibitors Selegeline (Eldepryl) Zelopar (Eldepryl Zydis) Rasagaline (Azilect) COMT Inhibitors Entacapone (Comtan) Tolcapone (Tasmar) Classes of Drugs For Parkinson’s Disease University Hospitals Neurological Institute
Progression of Parkinson’s Disease Early Moderate Advanced University Hospitals Neurological Institute
Early Stage • Diagnosis • Initiation of Therapy • Dopaminergic • Choice between dopamine Agonists and Levodopa based therapy • Other • MAOB-I, Amantadine, Anticholinergics • Education and Counseling • Identification and Treatment of Non-Motor Symptoms Patients generally do very well with medications given ~3X daily University Hospitals Neurological Institute
Moderate Stage • Emergence of motor complications • Early Wearing off • Morning Akinesia (hard to turn on in the morning) • On/Off Fluctuations • Dose Failures • Dyskinesia • Good control possible but more challenging and requires utilization of different medications and strategies University Hospitals Neurological Institute
Advanced Stage • Motor complications persist and more challenging • Emergence of treatment refractory symptoms • Balance Impairment • Cognitive Decline • Autonomic Dysfunction University Hospitals Neurological Institute
Early Wearing Off • Brain cells in substantia nigra - Cells that make and store dopamine in the brain are progressively lost in PD • 70% are lost before symptoms are obvious • Half-life of Levodopa is 90 minutes • But in early disease even levodopa based medications last 6-8 hours—Why? • Levodopa is recycled by the brain – in substantia nigra • With loss of these cells, duration of response to levodopa becomes shorter and shorter University Hospitals Neurological Institute
Dyskinesia • Intermittent dosing of levodopa leads to pulsatile stimulation of brain dopamine receptors • Pulsatile stimulation is believed to lead to the development of dyskinesia Dopamine Levels Dose University Hospitals Neurological Institute
Dose Failures • Levodopa’s PK profile is characterized by • very short plasma half-life due to rapid metabolism • variability in GI absorption due to: • GI dysmotility secondary to PD, delayed gastric emptying • Inhibition of transport across the gut–blood barrier • potential delays in blood–brain barrier transport Blood Brain GI System GI Dysmotility Protein Interference Protein Interference University Hospitals Neurological Institute
Pharmacological Approaches to Motor Complications University Hospitals Neurological Institute
Comparison of Oral Dopaminergic Medications University Hospitals Neurological Institute
Oral Dopamine Agonists (ropinerole, pramipexole) levodopa/carbidopa levodopa/carbidopa + dopamine agonist • Much longer half life — 5-8hrs vs. 90 min • Allows for smoother control with milder offs • May reduce levodopa dose University Hospitals Neurological Institute
COMT Inhibition (entacapone, tolcapone) • Blocks the breakdown of levodopa and increases the duration of action by 30-60 minutes • Comtan(entacapone) dosed frequently up to 8 times a day • May be combined in 1 pill with levodopa/carbidopa as Stalevo University Hospitals Neurological Institute
MAO-B Inhibitors (selegeline, rasagiline) • Blocks breakdown of dopamine • Increases effect of own dopamine • Increases effect and smoothes therapeutic effect of levodopa/carbidopa • Effect of medication lasts several days but requires daily dosing University Hospitals Neurological Institute
Dose Fractionation • Can smooth levels and reduce off time and dyskinesia by reducing levodopa dose and increase frequency University Hospitals Neurological Institute
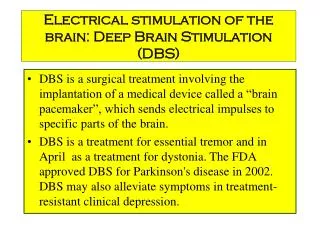
DBS for Movement Disorders Patient Selection and Evaluation University Hospitals Neurological Institute
Deep Brain Stimulation Surgery Stage I Stage II University Hospitals Neurological Institute
Who is a candidate? • “Idiopathic” Parkinson’s disease • Originally good response to Sinemet • No longer satisfied with response from medication due to any of the following: • Shortened or unpredictable medication response • Tremor • Stiffness • Slowness • Dyskinesia • No significant depression, anxiety or memory loss • . University Hospitals Neurological Institute
Our thought process . . . • Does the patient have “Idiopathic PD” • What does the patient expect to get from surgery? – Is it something surgery will help? • Have medications been tried adequately? • How do the predictors for good and bad outcome weigh in the patient? University Hospitals Neurological Institute
When are medications not enough? • Despite medication adjustments patient still has: • Early wearing off before next dose of medication • Frequent cycling between on and off • Tremor refractory to medication • Troubling dyskinesias University Hospitals Neurological Institute
What are realistic expectations from surgery? • Improved Tremor • Improved Dyskinesia • Less ups and downs • Longer lasting benefit through the day • Improved slowness • Improved dystonia (cramps) • Some reduction in medication • Improved off freezing University Hospitals Neurological Institute
What are not realistic expectations from surgery? • Improved “on-freezing” • Improved balance • Improved memory • Improved swallowing, or bladder function University Hospitals Neurological Institute
Predictors of Good Outcome • Good response to Sinemet or other dopaminergic therapies • Early wearing off, fluctuations between on and off • Dyskinesias • Tremor University Hospitals Neurological Institute
Predictors of Poor Outcome • Poor response to Sinemet (except tremor) • Hallucinations • Significant memory loss, depression or anxiety • Early problems with memory, low blood pressure, swallowing, bladder control or hallucinations. University Hospitals Neurological Institute
What is most important! • The patient gets from surgery what they anticipated from it University Hospitals Neurological Institute
What can be done to optimize the outcome? • Multi-specialty evaluation • Identify patients with significant memory loss • Identify and treat untreated or undertreated depression and anxiety • Weigh risks and benefits of implanting one side or both University Hospitals Neurological Institute
Sites for Stimulation • Subthalamic Nucleus (STN) • Globus Pallidus Internus (GPi) University Hospitals Neurological Institute
University Hospitals Movement Disorders Team University Hospitals Neurological Institute
Contact Us Appointment Line: (216) 844-3192 Office: (216) 368-5247 Questions about DBS: Christina Whitney, PhD, ACNS-BC (216) 844-8542 University Hospitals Neurological Institute
Thank You. University Hospitals Neurological Institute