Download
1 / 40

E N D
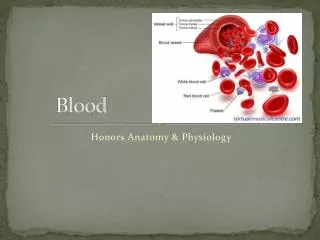
General Components of Blood • Whole Blood can be broken into 2 main components: • Plasma (46-63%) • Formed elements (37-54%). Plasma itself consists primarily of: • Water (92%) • Plasma Proteins (7%) • Other solutes (1%). • The formed elements consist of: • Red blood cells (99.9%) • White blood cells (>0.1%) • Platelets (>0.1%).
Functions of the blood • Blood performs two major functions: • transport through the body of • oxygen and carbon dioxide • food molecules (glucose, lipids, amino acids) • ions (e.g., Na+, Ca2+, HCO3−)(carboxylic acid) • wastes (e.g., urea) • hormones • heat • defense of the body against infections and other foreign materials. All the WBCs participate in these defenses.
Other functions of blood. They include: • Transport of dissolved gases, nutrients, hormones, and metabolic wastes. • Regulation of the pH and electrolyte composition of interstitial fluids throughout the body. • Restriction of fluid losses (in event of injury). • Defense against toxins and pathogens.
Composition of PlasmaPlasma is the straw-colored liquid in which the blood cells are suspended. It is the liquid portion of the blood
Serum Proteins ( in the Plasma ) • Proteins make up 6–8% of the blood. They are about equally divided between serum albumin and a great variety of serum globulins. • After blood is withdrawn from a vein and allowed to clot, the clot slowly shrinks. As it does so, a clear fluid called serum is squeezed out. Thus: • Serum is blood plasma without fibrinogen and other clotting factors.
Formation of different types of blood cells from stem cells.
A red blood cell • Red blood cell synthesis is known as erythropoiesis. In the adult, all blood cell formation (i.e., synthesis of RBCs, WBCs, and platelets) occurs in the red bone marrow.
RED BLOOD CELL FORMATION ( Erythropoiesis ) • In health, erythropoiesis is regulated so that the number of circulating erythrocytes is maintained within a narrow range. Normally, a little less than l% of the body's total red blood cells are produced per day and these replace an equivalent number that have reached the end of their life span. However that still represents a huge 200,000,000,000 cells • Erythropoiesis is stimulated by hypoxia (lack of oxygen). However, oxygen lack does not act directly on the haemopoietic tissues but instead stimulates the production of a hormone, erythropoietin. This hormone then stimulates haemopoietic tissues to produce red cells. • Erythropoietin is a glycoprotein. It is inactivated by the liver and excreted in the urine. It is now established that erythropoietin is formed within the kidney by the action of a renal erythropoietic factor erythrogenin. • Erythrogenin is present in the juxtaglomerular cells of the kidneys and is released into the blood in response to hypoxia in the renal arterial blood supply. • Various other factors can affect the rate of erythropoiesis by influencing erythropoietin production.
What happens to the iron? Iron will be stored in the liver as well as transported to red bone marrow (to be incorporated in new RBCs) and other tissues Iron is transported in the blood as a protein complex called transferrin and stored within liver cells.
Hematocrit • An essential test used to examine blood is the hematocrit. The hematocrit is a measure of the percentage of whole blood occupied by RBCs. • Average value in a male is 47% (range of 42-52%). • Average in a female is 42% (range of 37-47%). • HCT can be determined by centrifuging a sample of blood so that all the formed elements come out of suspension - we will do this in lab! • Since leukocytes and platelets make up far less than 1% of the blood, it can be assumed that: (100-HCT) = % of blood occupied by plasma.
Types of WBCs: • They can be classified as to whether or not they contain granules that take up Wright's stain and are visible with the light microscope. • Granulocytes • Contain visible stained granules. Includes: • Basophils • Eosinophils • Neutrophils. • Agranulocytes • Do not contain stained visible granules. Includes: • Lymphocytes • Monocytes.
- 50-70% of circulating WBCs. - Cytoplasm is packed with pale "neutral" colored granules that contain bactericidal compounds.- Mature neutrophils have a segmented nucleus - and are thus known as polymorphonuclear leukocytes.- About 12um in diameter.- Highly mobile and generally the first WBCs to arrive at a site of injury.- Specialize in attacking and digesting bacteria that have been "marked" for destruction.- Lifespan of about 6hrs to a few days. Neutrophils
Eosinophils • 2-4% of circulating WBCs. • Similar in size to neutrophils but have reddish-orange staining granules. • Functions: • Phagocytize antibody-coated bacteria, protozoa, and cellular debris. • Exocytose toxic compounds onto the surface of pathogens, particularly large multicellular parasites such as flukes or parasitic worms. • They increase in # dramatically during a parasitic infection. • Also sensitive to allergens and increase in # during allergic reactions as well. • Typical lifespan of 8-12d.
Basophils • Less than 1% of circulating leukocytes. • Smaller than eosinophils and neutrophils. • Contain granules that appear deep purple or blue. • Migrate to injury sites and discharge the contents of their granules: • Histamine • Vasodilator and increaser of capillary permeability. • Heparin • An anticoagulant. • These 2 chemicals enhance the local inflammation initiated by mast cells and attract other WBCs. • Lifespan is not certain.
Monocytes • 2-8% of circulating WBCs. • Almost 2x as big as an RBC. • Nucleus is large & tends to be oval or kidney-shaped. • Individual monocytes use the bloodstream as a highway, staying in the circulation for only about 24hrs before an entering peripheral tissues to become a tissue macrophage, an aggressive phagocyte. • Lifespan can be up to several months.
Lymphocytes • 20-30% of circulating WBCs. • Slightly larger than RBCs. • In blood smears, you typically only see a thin halo of cytoplasm around a relatively large nucleus. • Continuously migrate from the bloodstream into the peripheral tissues and back into the bloodstream. • Circulating lymphocytes are only a minute fraction of the total # in the body. Most are in other connective tissues and in lymphatic organs. • Circulating blood contains 2 main classes of lymphocytes: • T Lymphocytes: Defend against foreign cells and tissues and coordinate the immune response. • B Lymphocytes: Produce and distribute antibodies - proteins that attack foreign molecules. • Lifespan of hrs to yrs.
Hemoglobin (Hgb) Men:14–18 grams per deciliter (g/dL) or 8.7–11.2 mmol/L (SI units) Women:12–16 g/dL or 7.4–9.9 mmol/L Red blood cell (RBC) count Hematocrit (HCT)
Red blood cell indices Mean corpuscular volume (MCV): 80–100 femtoliters (fL) Mean corpuscular hemoglobin (MCH): 28–32 picograms (pg) Mean corpuscular hemoglobin concentration (MCHC): 32–36 grams per deciliter (g/dL)
WBC count: 4,500–11,000/μL • polymorphonuclear neutrophils: 1800–7800/μL; (50–70%) • band neutrophils: 0–700/μL; (0–10%) • lymphocytes: 1000–4800/μL; (15–45%) • monocytes: 0–800/μL; (0–10%) • eosinophils: 0–450/μL; (0–6%) • basophils: 0–200/μL; (0–2%)
Platelets • Platelets are cell fragments produced from megakaryocytes. Blood normally contains 150,000–350,000 per microliter (µl) or cubic millimeter (mm3). This number is normally maintained by a homeostatic (negative-feedback) mechanism . • If this value should drop much below 50,000/µl, there is a danger of uncontrolled bleeding because of the essential role that platelets have in blood clotting. • Platelets contains chemical substances or blood factors which play a major role in blood clotting.
The production of platelets is called thrombopoiesis • Flattened, disk-like cell fragments that are about 1um by 4um. • Act as a participant in the vascular clotting system. • Sometimes referred to as thrombocytes. • Continuously being replaced. Each platelet circulates for 9-12 days before being removed by splenic macrophages. • On average there are 350,000 platelets per uL of blood. • Produced in the bone marrow. Large cells called megakaryocytes release fragments (platelets) into the circulation
This looping diagrammatic animation shows the process of platelet formation from a megakaryocyte
What do platelets do? • Transport of chemicals integral to the clotting process. • By releasing enzymes and other factors, platelets help initiate the clotting process. • Formation of a temporary patch (called a platelet plug) in the wall of a damaged blood vessel.
Blood clotting • Vascular Phase • Damage to the wall of a blood vessel will obviously affect those cells that comprise the wall. • The endothelial cells (simple squamous epithelium that lines the blood vessel lumen) at the site of an injury will: • Have their basement membrane exposed. • Release a variety of chemicals. • Become "sticky." • The smooth muscle cells in the blood vessel wall also respond to damage. They CONTRACT. By contracting, the blood vessel diameter decreases which helps to reduce blood loss and reduce the pressure on the damaged area.
Platelet Phase • Platelets begin to attach to the sticky endothelial cells, the basement membrane, and to exposed collagen fibers. • As platelets "stick," they are activated and they release chemicals that: • Attract and activate more platelets. • Cause local vasoconstriction (contraction of blood vessel smooth muscle and a subsequent decrease in the diameter of the blood vessel lumen). • Eventually, we are left with a mass of platelets that temporarily plugs the leak in the damaged blood vessel wall. • It should be noted that intact endothelial cells release a chemical called prostacyclin which inhibits platelet aggregation. This restricts the plug to the site of the damage.
Coagulation Phase • Now we need to create a more permanent seal that can effectively cover the break while repairs take place. In other words, we need a clot. • The coagulation phase is a sequence of chemical reactions that culminate in the conversion of fibrinogen (a soluble circulating plasma protein made by the liver) into a meshwork of the insoluble protein fibrin. • The fibrin meshwork will grow and cover the surface of the platelet plug. RBCs and additional platelets are trapped in this tangle forming a blood clot that will effectively seal the walls of the damaged blood vessel. • Coagulation requires calcium as well as clotting factors - several different proteins primarily synthesized by the liver. • Many clotting factors are proenzymes (inactive enzymes) that have to be converted to active enzymes before they can direct essential reactions in the clotting process. • The synthesis of some of the clotting factors requires vitamin K. • During the coagulation phase enzymes and proenzymes interact. The activation of one proenzyme creates an active enzyme that activates another proenzyme that will then activate a third and so on yielding a chain reaction or cascade. You can think of it kind of like a row of dominos falling down.
There are actually 2 main cascades involved in the clotting process: the extrinsic pathway,and intrinsic pathway. • Extrinsic Pathway • Begins with the release of tissue factor by damaged endothelial cells or peripheral tissues. • The greater the damage, the more tissue factor released, and the faster clotting will occur. • In a few short steps, a chemical called prothrombin activator will have been formed. Because only a few steps are required, the extrinsic path forms prothrombin activator rather quickly. • Intrinsic Pathway • Begins with the exposure of collagen which starts the activation cascade of several proenzymes eventually resulting in the production of prothrombin activator. • Because there are several steps, the intrinsic path does not make prothrombin activator as fast as the extrinsic path. However, multiple steps allows for more amplification which means more prothrombin activator will be made.
How do we get rid of the clot? • Fibrinolysis • As repairs proceeds, the clot gradually dissolves. This dissolution is known as fibrinolysis. • Fibrinolysis begins with the activation of the proenzyme plasminogen by 2 enzymes: • Thrombin activated in the common pathway. • Tissue plasminogen activator released by damaged tissue. • Once plasminogen is turned into plasmin, the plasmin digests the fibrin strands and erodes the foundation of the clot. ______________________________________________ Plasmin BLOOD CLOT ---------------------------- clot dissolved