Download
1 / 9
100 likes | 390 Vues
Drugs affecting neuromuscular transmission. Professor Ian Hughes, 9.83; i.e.hughes@leeds.ac.uk motor nerve - skeletal (striated) muscle ONLY

E N D
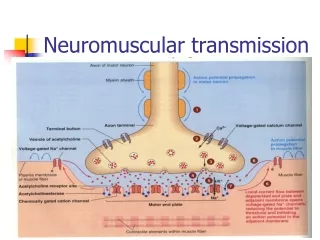
Drugs affecting neuromuscular transmission • Professor Ian Hughes, 9.83; i.e.hughes@leeds.ac.uk • motor nerve - skeletal (striated) muscle ONLY • single long cell from CNS; action potential (Na channels) invades terminal opening Ca channels; intracellular Ca rises; vesicles release ACh by exocytosis; diffusion to receptors (ligand operated ion channel [2xalpha,beta,gamma,delta]); Na flows out; depolarisation of endplate; if sufficient depolarisation then voltage operated Na channels open and a propogated action potential followed by contraction results in muscle.
choline recapture Choline acetylcholine esterase choline acetylase action potential R ACh (10,000) in vesicle ACh - + Ca++ pre- synaptic receptors calcium entry diffusion
Pre-synaptic actions • block nerve action potential; lignocaine • prevent choline uptake; hemicholinium triethylcholine • block choline acetylase • affect release mechanism; Ca++ entry excess Mg++ ; botulinus toxin; • affect pre-synaptic receptors; • discharge vesicles; beta bungarotoxin ; black widow spider venom • affect potassium channels;4-aminopyridine; TEA
Post-synaptic actions • competitive blockers; tubocurarine, pancuronium, gallamine, fazadinium, atracurium, vecuronium • depolarising blockers; suxamethonium (succinylcholine) • odds and sods; decamethonium, dantroline
Competitors (Tc) and depolarisers (Sux) - mechanism of action mV map epp . . . . . . Sux [Tc] stim
Compare:--------------------------------competitors -- depolarisers • fasciculations no yes • paralysis (man) flaccidflaccid • paralysis (bird) flaccidspastic • tetanic stimulation fades maintain • anticholinesterase reversedeepen • K channel blocker reversedeepen • +depolariser reversedeepen • +competitor deepenreverse • multiply innervated --------- contracts muscle
Uses of neuromuscular blockers • entubation- fast and short action • relaxation during surgery- long action, reversible, controlled • soften electro-convulsive therapy- short and fast action (use with anaesthetic) • special conditions- renal or hepatic failure; manipulations; exceptionally convulsions.
Drugs • tubocurarine- quaternary; release histamine;some ganglion block hence BP falls; hepatic 70%, renal 30%; 30-40 min • pancuronium - longer lasting; renal 75% • vecuronium - short (20 min); hepatic 85%, renal 15% • gallamine - renal 90%; 30-40 min • fazadinium - short; hepatic 90% (diazo reduction) • atracurium - short; pH dependent chemical destruction • rocuronium, mivacurium
Drugs • suxamethonium - (Scoline); depolariser; short (3-10min); scoline pains and muscle damage; K+ levels increased; dysrhythmias; hydrolysed by esterases (defect). • decamethonium - initial depolarising, later competitive characteristics; longer lasting. • dantroline - acts to inhibit Ca++ release in muscle; used in malignant hyperthermia and severe muscle spasm.