Download
1 / 55
570 likes | 832 Vues
Pharmacology of Coagulation. Outline. I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation. Outline. I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation. Blood exhibits laminar flow in an intact vessel. A. Laminar.

E N D
Outline I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation
Outline I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation
Blood exhibits laminar flow in an intact vessel. A Laminar flow EC Collagen fibers
Platelets become activated if a vessel wall breaks. B vWF EC Collagen fibers GPIb GPIa/IIa
Platelets become activated if a vessel wall breaks. C EC Collagen fibers vWF 5-HT ADP TA2 ADP TA2 5-HT vWF TA2 activates GPIIb/IIIa receptors, allowing them to bind fibrinogen. GPIIb/IIIa TA2 recruits more platelets by activating GPIIb/IIIa receptors. TA2 activates platelet surface. TA2 causes release of platelet granules. vWF binds to GPIIb/IIIa receptors
Thrombin produced as a result of clot initiation also activates platelets. A EC Collagen fibers Smooth muscle cell Tissue factor activation VIIa VIIa Thrombin X Xa Prothrombin
As a result of the propagation phase, thrombin produces enough fibrin for a clot. B EC Collagen fibers Fibrin a I I I X a I X V Prothrombin Thrombin a I X I I a a V I V I I Xa a Fibrinogen
This picture illustrates how factors and cofactors interact on the platelet surface. From: Robbins Basic Pathology, 8th Ed.
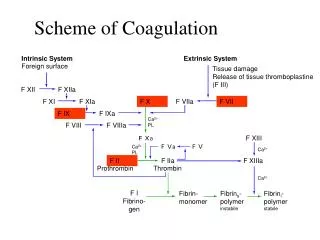
The coagulation cascade consists of extrinsic (most important in vivo) and intrinsic pathways. Intrinsic XIIa XII Extrinsic XIa XI TF + VIIa TF-VIIa Platelet IX IXa VIIIa VIII Xa X Va V Prothrombin Thrombin XIII Fibrinogen Fibrin XIIIa
Outline I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation
The body has numerous methods to prevent coagulation and to remove clots. There must be a balance between clotting and anti-clotting mechanisms. Anti-clotting mechanisms: Inhibit platelet aggregation Block formation of thrombin Inactivate thrombin after it has formed Remove clots by producing plasmin to destroy fibrin
PGI2 and NO both inhibit platelet aggregation. A PGI2 NO NO PGI2 EC Collagen fibers
TFPI binds to and inhibits the action of the TF-VIIIa complex. Intrinsic XIIa XII Extrinsic XIa XI TF + VIIa TF-VIIa X Platelet TFPI X IX IXa VIIIa VIII Xa X Va V Prothrombin Thrombin XIII Fibrinogen Fibrin XIIIa
Thrombomodulin inactivates thrombin, and allows thrombin to activate protein C which then binds protein S. B S S C C Thrombin Thrombin EC Collagen fibers Thrombin binds to thrombomodulin, inactivating thrombin. The inactivated thrombin can now bind protein C, activating protein C. Activated protein C now binds protein S. Proteins C and S can now affect factors Va and VIIIa (next slide).
Proteins C and S inactivate factors Va and VIIIa. Intrinsic XIIa XII Extrinsic XIa XI TF + VIIa TF-VIIa X Platelet TFPI X IX IXa CS VIIIa VIII Xa X CS Va V Prothrombin Thrombin XIII Fibrinogen Fibrin XIIIa
Antithrombin in the presence of heparan inactivates thrombin and factors IXa and Xa. Thrombin B IXa Xa S S C C AT AT Thrombin Thrombin H H EC Collagen fibers
Tissue plasminogen activator (t-PA) and urokinase activate plasmin which destroys fibrin. C Plasminogen Plasmin t-PA urokinase EC Collagen fibers Fibrin Plasmin is activated from plasminogen, and dissolves clots. t-PA (from EC) and urokinase (from kidney) are plasminogen activators. Plasminogen, t-PA, and urokinase are incorporated into clots. Balance of clot initiators and clot dissolvers determines duration of clot.
Outline I. Coagulation Cascade II. Anti-Clotting Mechanisms III. Drugs Affecting Coagulation
Heparin acts similarly to heparan. It has varying molecular weights: unfractionated (UFH) or high-molecular weight (HMW) to low-molecular weight (LMH). Similar to heparan, it facilitates action of antithrombin to inactivate thrombin and factors IXa and Xa.
Heparin acts similarly to heparan. Thrombin B IXa Xa S S C C AT AT Thrombin Thrombin H H EC Collagen fibers
Heparin acts similarly to heparan. It has varying molecular weights: unfractionated (UFH) or high-molecular weight (HMW) to low-molecular weight (LMH). Similar to heparan, it facilitates action of antithrombin to inactivate thrombin and factors IXa and Xa. Patients on UFH must be monitored with aPTT. LMW mainly inhibits Xa, and not as necessary to monitor unless patient is pregnant, has renal insufficiency, or is obese.
Heparin has predictable uses and adverse effects. Used to treat people with thromboses or those likely to develop thromboses Can be used in pregnancy Given parenterally, iv initially but then subcutaneously Primary adverse effect is bleeding (DUH!), counteracted by protamine sulfate. Heparin can induce thrombocytopenia Osteoporosis may occur with chronic use
These are the heparin preparations. Enoxaparin (Lovenox), dalteparin (Fragmin), tinzaparin are LMW heparins. Danaparoid is similar to heparan. Fondaparinux (Arixtra) is synthetic and inhibits only factor Xa, less likely to induce thrombocytopenia. Can be used in people who already have heparin-induced thrombocytopenia. LMWs are used more commonly because of predictable effects, but protamine doesn’t work as well, and doesn’t work at all to reverse effects of danaparoid and fondaparinux.
Warfarin prevents synthesis of clotting factors that require vitamin K. Prothrombin is the example in this figure. Prothrombin is carboxylated in a reaction that converts reduced vitamin K (KH2) to vitamin K epoxide (KO). To be used again, KO must be reduced to KH2. Warfarin blocks vitamin K epoxide reductase, preventing the reduction of KH2.
Warfarin prevents synthesis of clotting factors that require vitamin K. Warfarin (Coumadin): Prevents synthesis of prothrombin, proteins C and S, and factors VII, IX, and X.
Warfarin prevents synthesis of clotting factors that require vitamin K. Intrinsic XIIa XII Extrinsic XIa XI X TF + VIIa TF-VIIa X Platelet TFPI X X IX IXa X CS VIIIa VIII X Xa X X CS Va V X Prothrombin Thrombin XIII Fibrinogen Fibrin XIIIa
Warfarin prevents synthesis of clotting factors that require vitamin K. Warfarin(Coumadin): Used to treat thromboses; often given after initial heparin Given orally. PT and INR used for monitoring. Main adverse effect is bleeding; giving vitamin K can reduce bleeding Skin necrosis may occur during first few weeks. Contraindicated in pregnancy
Warfarin interacts with many drugs. Prolong bleeding time: Inhibit metabolism of warfarin: amiodarone, cimetidine, disulfiram, metronidazole, fluconazole, trimethoprim-sulfamethoxazole Aspirin and heparin: By their own anticoagulant actions Third generation cephalosporins: Kill vitamin K-synthesizing bacteria and block vitamin K epoxide reductase. Hepatic disease, hyperthyroidism Reduce bleeding time: Barbiturates and rifampin enhance enzymatic destruction Cholestyramine prevents GI absorption Chlorthalidone and spironolactone reduce excretion of clotting factors Hypothyroidism reduces metabolism of clotting factors
Some drugs directly inhibit thrombin. Lepirudin (Refludan) is a recombinant form of hirudin (the active ingredient in leech spit) that binds to thrombin, inhibiting its action. Dabigatran (Pradaxa) is a recently approved (Oct, 2010) orally active drug that binds to thrombin.
Lepirudin and dabigatran inhibit thrombin. Intrinsic XIIa XII Extrinsic XIa XI TF + VIIa TF-VIIa X Platelet TFPI X IX IXa CS VIIIa VIII Xa X CS Va V X Prothrombin Thrombin XIII Fibrinogen Fibrin XIIIa
Lepirudin’s main disadvantage is that it has to be administered parenterally, usually IV. Lepirudin (Refludan): Used to treat thrombosis in people with heparin-induced thrombocytopenia or unstable angina. Administered IV
As usual, the major adverse effect of lepirudin is bleeding. Similar to lepirudin are bivalirudin and argatraban. All three drugs must be monitored with PTT. Lepirudin is no longer manufactured; supply should be gone by June, 2013.
Dabigatran is the first of several new anticoagulants that probably will change treatment of coagulation disorders. Dabigatran (Pradaxa) is currently approved for treating non-valvular atrial fibrillation. A major advantage of dabigatran is that blood monitoring is not required. Dabigatran is taken orally twice daily. The major adverse effect is (ta-da!): bleeding!
Streptokinase and alteplase are fibrinolytic. Streptokinase (Streptase) and alteplase (Activase): Facilitate the formation of plasmin from plasminogen, dissolving fibrin
Streptokinase and alteplase enhance the formation of plasmin. C Plasminogen Plasmin t-PA urokinase EC Collagen fibers Fibrin
Streptokinase and alteplase are given parenterally. Streptokinase (Streptase) and alteplase (Activase): Used for arterial thrombotic conditions. Given IV or intra-arterially Major adverse effect is, again, bleeding. Overdoses can be treated with aminocaproic acid which inhibits plasminogen activation.
Some drugs inhibit platelets. Antiplatelet drugs: Inhibit activation of platelets
Aspirin irreversibly inhibits platelets. Irreversible inhibitors Aspirin: Irreversibly binds cyclooxygenase, preventing synthesis of thromboxane A2
By irreversibly binding to COX, aspirin prevents the formation of thromboxane A2. Tissue Damage Disruption of cell membranes Phospholipids in cell membranes Phospholipase A 2 Arachidonic acid COX-1 and COX-2 Lipoxygenase pathways PGG 2 PGH 2 PGD PGE PGF Prostacyclin (PGI ) Thromboxane A 2 2 a 2 2 (from mast cells) (from many sources) (from uterus) (from endothelial cells) (from platelets) Vasodilation Uterine contraction Vasodilation Vasoconstriction Increase vascular permeability Inhibit platelet aggregation Increase platelet aggregation from Anti-inflammatory drugs lecture in DDT
By irreversibly binding to COX, aspirin prevents the formation of thromboxane A2. C EC Collagen fibers ADP X TA2 5-HT GPIIb/IIIa
Clopidogrel blocks the ADP receptor on platelets. Irreversible inhibitors Clopidogrel (Plavix), ticlopidine (Ticlid), and prasugrel (Effient) block ADP receptors, reducing platelet activation.
Clopidogrel blocks the ADP receptor on platelets. C EC Collagen X fibers ADP TA2 5-HT GPIIb/IIIa
Abciximab binds to the GP IIb/IIIa receptors. Irreversible inhibitors Abciximab (ReoPro) binds to the GP IIb/IIIa receptors, preventing platelet aggregation by blocking attachment of fibrinogen and von Willebrand factor to platelets.
Abciximab prevents binding of fibrinogen and von Willebrand factor to platelets. C EC Collagen fibers ADP TA2 5-HT X X GPIIb/IIIa X X
Eptifibatide and tirofiban also bind the GP IIb/IIIa receptor, but inhibition is reversible. Reversible inhibitors Eptifibatide (Integrilin) and tirofiban(Aggrastat): Bind to GP IIb/IIIa receptor, blocking fibrinogen binding
Cilostazol inhibits platelet aggregation. Reversible inhibitors Cilostazol(Pletal): Blocks PDE III, inhibiting platelet aggregation
Major uses of antiplatelet drugs relate to cardiovascular diseases. Clinical uses: Prevention of myocardial infarction: aspirin, abciximab, eptifibatide, tirofiban Prevention of transient ischemia attacks and stroke: aspirin, clopidogrel, ticlopidine Prevention of restenosis after stents: aspirin, abciximab, eptifibatide, tirofiban, clopidogrel, ticlopidine Intermittent claudication: aspirin, cilostazol
Blood and more blood! Administration: Aspirin and clopidogrel: Orally Others: Parenterally Adverse effects: Dare we ask the main adverse effect???
A new class of anticoagulants blocks factor Xa. Rivaroxaban(Xarelto) and apixaban (Eliquis) inhibit factor Xa. Both are approved to reduce the likelihood of thromboses in non-valvular atrial fibrillation. Rivaroxaban also is approved to prevent venous thromboses after hip and knee surgery, and to treat deep vein thrombosis. Do not require monitoring. The major adverse effect is bleeding for which there is no antidote.