Download
1 / 54
540 likes | 542 Vues
This text provides an overview of the respiratory system, discussing the different areas of the oral cavity, the lower respiratory tract, and the larynx. It covers the anatomy and function of each component, including the trachea, vocal cords, and various cartilages. The text also touches on common respiratory conditions such as acute and chronic laryngitis.

E N D
Respiration begins in the nose Ciliated columnar epithelial tissue lines the nose to warm and mositen the inhaled air. Mucous cells are found within the lining to allow moistening of the air.
3 Areas of the Oral Cavity • OROPHARYNX -soft palate to epiglottis -two sets of TONSILS a. Palatine b. Lingual -the tonsils remove pathogens that enter the pharynx. They contain lymphocytes
2. NASOPHARYNX -located superior and posterior to the soft palate. -contains the PHARYNGEAL TONSILS and TUBAL TONSILS
The soft palate is a muscular structure that separates the nasal cavity from the oral cavity. The soft palate moves superiorly to seal the nasal cavity during swallowing.
An 11-month-old girl's mother noted this asymptomatic cyst on her daughters soft palate.
3. LARYNGOPHARYNX -inferior to the epiglottis and posterior to the larynx. - this division opens into the esophagus and larynx.
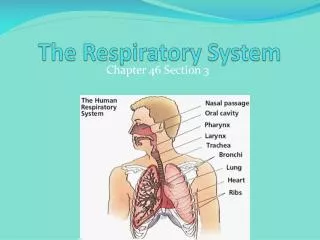
The Lower Respiratory Tract • The TRACHEA begins at the level of C6 superiorly. • Directly superior to the beginning of the trachea is the LARYNX (vocal cords). • The trachea bifurcates into the BRONCHI at the sternal angle (T4 or T5) when supine (laying on the back) or T7 when standing.
The trachea is composed of 16-20 cartilagenous rings (hyaline cartilage). • These rings are flexible but keep the trachea open. • Each ring is open in the back (allows flexibility)
The rings are approximately 1.5 inches in diameter and held together by connective tissue. • The connective tissue is dense CT. • Air can pass through the tube without resistance.
The trachea must be able to filter debris (dust or dirt). Coughing occurs when such debris enters the trachea. • This coughing is due to the CILIATED EPITHELIUM which lines the trachea.
Histology of the trachea Ciliated epithelium cartilage
The Larynx • The LARYNX (voice box) is a modified portion of the trachea. • It is superior to the trachea. • There are cartilaginous rings that are connected by dense connective tissue forming a tube.
The TYROID CARTILAGE is shaped like a shield when viewed from the anterior surface. This is the ADAM’S APPLE. This is not a complete ring. • On the posterior side of the thyroid cartilage, the CRICOID CARTILAGE extends superiorly to where the thyroid cartilage would be. This cartilage is sometimes called the SIGNET RING CARTILAGE.
It has a narrow band across the anterior side. • It is superficial to the thyroid cartilage posteriorly where it is connected by the CRICOTHYROID LIGAMENT (dense connective tissue). • Inferiorly, the cricoid is attached to the first ring to the trachea by dense CT.
The EPIGLOTTIS is a spade shade cartilage that is important during swallowing. • It tips inferiorly to seal off the glottis and prevents food from entering the trachea. • The ARYTENOID CARTILAGE is below the epiglottis at the entrance to the GLOTTIS. • The GLOTTIS is a passageway into the trachea. The thyroid cartilage forms the walls of the glottis. The arytenoid cartilage extends inferiorly into the glottis.
The arytenoid cartilages anchor the vocal cords. • The true vocal cords are located inferiorly inside the glottis. • As air passes over the vocal cords they flutter, producing sound from the vibration. • Pitch can be changed by tightening or loosening the cords. • In humans, the tongue is used to make sense of the sounds (make words). You cannot talk if your tongue is not functioning. • There are folds covering part of the epiglottis called FALSE VOCAL CORDS.
Epiglottis Hyoid Bone ThyrohyoidLigament Thyroid Cartilage Aryetnoid cartilage Cricoid cartilage ANTERIOR trachea Tracheal rings POSTERIOR
Step 2 The skin incision is made with a Colorado Needle mounted on an electric knife (Bovie). A steel blade scalpel is as good and is preferred by many surgeons.
Step 3 After incising the subcutaneous tissue and platysma, the strap muscles are separated in the midline. The strap muscles is a name given to the four infrahyoid muscles that lie in front of the larynx. They are the sternohyoid, sternothyroid, thyrohyoid and the omohyoid.
Step 4 The isthmus of the thyroid gland is either retracted or divided in the midline. (In this picture, the isthmus has been divided and retracted laterally, along with the strap muscles.) The anterior tracheal wall is divided between the third and fourth tracheal rings. A clamp is used to widen the tracheal opening. The endotracheal tube is seen inside the tracheal lumen
Normal vocal cords as they appear through a 90 degree telescope. The cords are partially opened and the opening into the trachea can be seen between them.
One may compare this person at a high and a low pitch, demonstrating the elongation of the vocal cords that takes place to raise pitch by contracting the Cricothyroid muscles
Chronic Laryngitis 68 year old non-smoker with history of gastroesophageal reflux. She complained of daily belching and burning in her throat due to the stomach acids.
Wider, shorter, and more vertical than the left trachea Right Primary Bronchus Left primary bronchus Both primary bronchi have the same anatomic structure as the trachea.
The primary bronchi divide to form SECONDARY BRONCHI (lobar bronchi). • There is one secondary bronchus for each lobe of the lungs. • There are 2 lobes on the left lung. • There are 3 lobes on the right lung. • These also have the same anatomy as the trachea.
The secondary bronchi branch to form TERTIARY BRONCHI. • They continue to branch. • As they get smaller, they lose their cartilage. • When they lose their cartilage, they are called BRONCHIOLES which are microscopic.
The bronchioles terminate in the ALVEOLI through an ALVEOLAR DUCT. • The walls of the alveoli are one-cell thick and is covered in capillaries. • The alveoli are the functional unit of the lungs.
There are air sacs, where gas exchange occurs. • Walls of the alveoli are highly vascularized. • The alveoli are the terminal branches of the BRONCHIAL TREE. This arrangement allows for a drastic increase in surface area.
The Lungs • The right lung starts 1” above rib 1 and crosses the clavicle at about the medial 1/3 of it. It progresses inferiorly to costal cartilage 6 (midsternally). At the midaxillary region, it is at rib 8 and rib 10 at the vertebral border.
The right lung has 3 lobes (4 in the cat). • The left lung starts about 1” above rib 1 and crosses deep to the manubrioclavicular joint. There it goes to the left and continues inferiorly to rib 6. • The left lung has an indentation called the CARDIAC NOTCH. This area provides room for the HEART.
Lung size varies from individual to individual. • The left lung has 2 lobes (3 in the cat). • The lobes are anatomically and functionally separate. Thus, they are independent of each other.
There is a deep fissure between the lobes. The lobes overlap each other like shingles. • The OBLIQUE FISSURE on each lobe begins posteriorly across from the root of the spine of the scapula at T3. They come around laterally and inferiorly in an oblique path and eventually reach rib 6 on both sides.
On the right side, there is also a TRANSVERSE FISSURE which follows rib 4 anteriorly. It joins the oblique fissure midaxillary. • On the posterior surface, one can see only 2 lobes on each lung. On the anterior surface, you can see the third lobe on the right lung.
The lobes are further divided into LOBULES. These cannot be separated as easily as the lobes can. • They are functionally separate. • They are also anatomically partitioned to allow removal of a lobule while keeping the functionality of the rest of the lung.
Gaseous exchange relies on simple diffusion. In order to provide sufficient oxygen and to get rid of sufficient carbon dioxide there must be • a large surface area for gaseous exchange • a very short diffusion path between alveolar air and blood • concentration gradients for oxygen and carbon dioxide between alveolar air and blood.