Download
1 / 1
10 likes | 137 Vues
Outcomes Following Adjuvant 5-FU based Treatment (AT) for Colon Cancer 1978-1995 vs. 1996-2007 Impact on Recurrence Rate, Time from Recurrence to Death (TRD) and Overall Survival (OS): Finding from the ACCENT Database

E N D
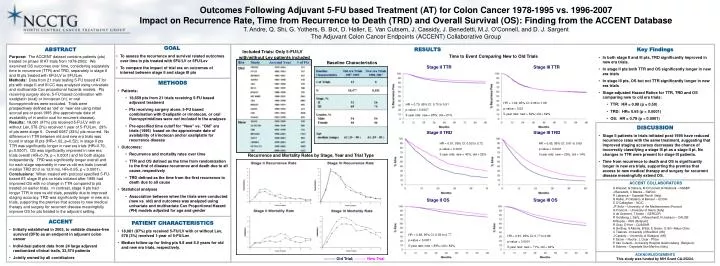
Outcomes Following Adjuvant 5-FU based Treatment (AT) for Colon Cancer 1978-1995 vs. 1996-2007 Impact on Recurrence Rate, Time from Recurrence to Death (TRD) and Overall Survival (OS): Finding from the ACCENT Database T. Andre, Q. Shi, G. Yothers, B. Bot, D. Haller, E. Van Cutsem, J. Cassidy, J. Benedetti, M.J. O’Connell, and D. J. Sargent The Adjuvant Colon Cancer Endpoints (ACCENT) Collaborative Group • GOAL • To assess the recurrence and survival related outcomes over time in pts treated with 5FU/LV or 5FU/Lev • To compare the impact of trial era on outcomes of interest between stage II and stage III pts ABSTRACT RESULTS • Key Findings • In both stage II and III pts, TRD significantly improved in new era trials. • In stage II pts both TTR and OS significantly longer in new era trials • In stage III pts, OS but not TTR significantly longer in new era trials • Stage-adjusted Hazard Ratios for TTR, TRD and OS comparing new to old era trials: • TTR: HR = 0.98 (p = 0.50) • TRD: HR= 0.65 (p < 0.0001) • OS: HR = 0.79 (p < 0.0001) Included Trials: Only 5-FU/LV with/without Lev patients included Time to Event Comparing New to Old Trials Purpose: The ACCENT dataset contains patients (pts) treated on phase III AT trials from 1978-2002. We examined OS outcomes over time, considering separately time to recurrence (TTR) and TRD, separately in stage II and III pts treated with 5FU/LV or 5FU/Lev. Methods: Data from 21 trials testing 5-FU based AT for pts with stage II and III CC was analyzed using univariate and multivariate Cox proportional hazards models. Pts receiving surgery alone, 5-FU based combination with oxaliplatin (oxal) or irinotecan (iri), or oral fluoropyrimidines were excluded. Trials were prospectively defined as ‘old’ or ‘new’ era using initial accrual pre or post-1995 (the approximate date of availability of iri and/or oxal for recurrent disease). Results: 18,081 (97%) pts received 5-FU/LV with or without Lev, 578 (3%) received 1 year of 5-FU/Lev. 29% of pts were stage II. Overall 6087 (33%) pts recurred. No difference in TTR between old and new era trials was found in stage III pts (HR=1.02, p=0.52); in stage II pts TTR was significantly longer in new era trials (HR=0.79, p=0.0007). OS was significantly improved in new era trials overall (HR=0.79, p < 0.0001) and for both stages independently. TRD was significantly longer overall and for each stage separately in new vs old era trials (overall median TRD 20.0 vs 12.8 mo, HR=0.65, p < 0.0001). Conclusions: When treated with protocol specified 5-FU-based AT, stage III pts on trials initiated after 1995 had improved OS with no change in TTR compared to pts treated on earlier trials. In contrast, stage II pts had longer TTR in new vs old trials, possibly due to improved staging accuracy. TRD was significantly longer in new era trials, supporting the premise that access to new medical therapy and surgery for recurrent disease meaningfully improve OS for pts treated in the adjuvant setting. Baseline Characteristics Stage II TTR Stage III TTR • METHODS • Patients: • 18,659 pts from 21 trials receiving 5-FU based adjuvant treatment • Pts receiving surgery alone, 5-FU based combination with Oxalipatin or irinotecan, or oral fluoropyrimidines were not included in the analyses • Pre-specified time cutoff for “New” vs. “Old” era trials (1995) based on the approximate date of availability of irinotecan and/or oxaliplatin for recurrence disease • Outcomes: • Recurrence and mortality rates over time • TTR and OS defined as the time from randomization to the first of disease recurrence and death due to all cause, respectively • TRD defined as the time from the first recurrence to death due to all cause • Statistical analyses • Association between when the trials were conducted (new vs. old) and outcomes was analyzed using univariate and multivariate Cox Proportional Hazard (PH) models adjusted for age and gender HR = 1.02, 95% CI: 0.96 to 1.08 p-value = 0.52 5-year rate: new = 62%; old = 62% HR = 0.79, 95% CI: 0.70 to 0.91 p-value = 0.0007 5-year rate: new = 85%; old = 81% • DISCUSSION • Stage II patients in trials initiated post-1995 have reduced recurrence rates with the same treatment, suggesting that improved staging accuracy decreases the chance of incorrectly classifying a stage III pt as a stage II pt. No changes in TTR were present for stage III patients. • Time from recurrence to death and OS is significantly longer in new era trials, supporting the premise that access to new medical therapy and surgery for recurrent disease meaningfully extend OS. Stage II TRD Stage III TRD HR = 0.61, 95% CI: 0.52 to 0.72 p-value < 0.0001 3-year rate: new = 43%; old = 25% HR = 0.65, 95% CI: 0.61 to 0.69 p-value < 0.0001 3-year rate: new = 29%, old = 14% Recurrence and Mortality Rates by Stage, Year and Trial Type ACCENT COLLABORATORS S Wieand, G Yothers, M O’Connell, N Wolmark – NSABP J Benedetti, C Blanke – SWOG R Labianca – Ospedali Riuniti (Italy) D Haller, P Catalano, A Benson – ECOG C O’Callaghan – NCIC JF Seitz – University of the Mediterranean (France) G Francini – University of Siena (Italy) A de Gramont, T Andre – GERCOR R Goldberg, L Saltz, J Meyerhardt, N Jackson – CALGB M Buyse – IDDI (Belgium) R Gray, D Kerr – QUASAR A Grothey, S Alberts, B Bot, E Green, Q Shi –Mayo Clinic C Twelves -University of Bradford (UK) J Cassidy – University of Glasgow (UK) F Sirzen – Roche ; L Cisar - Pfizer E Van Cutsem –University Hospital Gasthuisberg (Belgium); A Sobrero - Ospedale San Martino (Italy) Stage II OS Stage III OS • ACCENT • Initially established in 2003, to validate disease-free survival (DFS) as an endpoint in adjuvant colon cancer • Individual patient data from 24 large adjuvant randomized clinical trails, 33,574 patients • Jointly owned by all contributors • PATIENT CHARACTERISTICS • 18,081 (97%) pts received 5-FU/LV with or without Lev, 578 (3%) received 1-year of 5-FU/Lev • Median follow-up for living pts 9.8 and 6.0 years for old and new era trials, respectively. HR = 0.68, 95% CI: 0.59 to 0.77 p-value < 0.0001 5-year rate: new = 89%; old = 82% HR = 0.81, 95% CI: 0.77 to 0.86 p-value < 0.0001 5-year rate: new = 71%; old = 64% ACKNOWLEDGEMENTS This study was funded by NIH Grant CA-25224. ——— Old Trial; ——— New Trial