Download
1 / 62
700 likes | 1.22k Vues
Vascular Disorders. Acknowledgement is made to the following experts who contributed in the development of this module: Reina Kurrelmeyer, MBA, BSN, RN Leah Dicker, MSN, RN Albany Medical Center. November 2012. Objectives.

E N D
Vascular Disorders Acknowledgement is made to the following experts who contributed in the development of this module: Reina Kurrelmeyer, MBA, BSN, RN Leah Dicker, MSN, RN Albany Medical Center November 2012
Objectives Describe the pathophysiology of vascular disease Define treatment for vascular disease List at least three operative procedures to restore circulation to an affected extremity List three nursing interventions in the post operative management of vascular procedures
Overview Vascular Insufficiency Vascular Surgery Endovascular surgery Stenting techniques
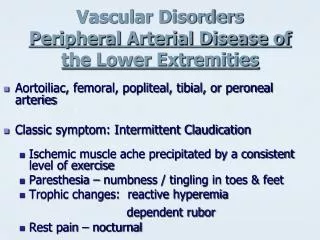
Vascular Insufficiency What is vascular insufficiency? Vascular insufficiency is a chronic condition that develops over time and is generally caused by: untreated or poorly controlled hypertension valve failure and backflow atherosclerotic lesions
Vascular Insufficiency Impaired blood flow eventually affects the lower extremities leading to clinical signs of vascular insufficiency, embolization and or thrombosis. Poor perfusion causes faint or absent pulses on exam and chronic to sharp pain in the affected extremity.
Vascular Insufficiency Poor perfusion will eventually lead to ischemia which may require surgical intervention in order to restore blood flow. Clots may also travel when dislodged, increasing the risk of a pulmonary embolism or stroke.
Vascular Insufficiency Clot formation seen on a leg with poor circulation due to vascular insufficiency.
Clot formation in the carotids.. Over 75% of strokes are caused by atherosclerotic changes in the carotid. When formed plaque dislodges it leads to cerebral ischemia. High risk populations include the elderly, males and African Americans. Other risk factors include hypertension, elevated cholesterol, smoking and ventricular enlargement.
Carotid Endarterectomy (CEA) A carotid endarterectomy is the surgical removal of plaque in an occluded carotid artery. It is typically performed in patients with significant stenosis (>60%). Plaque is removed through an incision in the neck and a JP drain is left in place to minimize hematoma formation.
Carotid Endarterectomy Post operative patients require specialized nursing care and serial assessments to prevent complications. Cardiovascular Continuous EKG monitoring w/ST segment elevation monitoring is recommended due to the potential for myocardial ischemia (intra-op or post-op).
Carotid Endarterectomy 2.Bradycardia- most commonly seen as a result of baroreceptor manipulation intra-op. Tight blood pressure management- to prevent vessel re-occlusion and promote hemodynamic stability.
Carotid Endarterectomy Neurological Frequent neurological checks should be performed in the immediate post operative period in addition to vascular checks. Inadvertent intra operative injury and possible dislodgment of plaque and or clots may lead to a stroke.
Vascular Endografts Endografts and stenting techniques have revolutionized the care of vascular patients. The procedures are less invasive than open surgery and offer an option to patients who are poor candidates for surgical repair.
Carotid Stenting Carotid stenting is performed on patients who are symptomatic, have had a recent stroke, have a >70% blockage AND are poor candidates for open surgical repair.
Carotid Stenting A stent is inserted into the carotid to increase blood flow in areas that are blocked by plaque. This plaque is typically caused by atherosclerosis which untreated can lead to TIAs and strokes.
Carotid Stenting Nursing assessments and care will be the same for CEAs and carotid stenting procedures as the risks are similar for the patient.
Endovascular procedures Abdominal Aortic Aneurysm (AAA) Thoracic Aortic Aneurysm (TAA) Endovascular Aneurysm Repair (EVAR) Thoracic Aneurysm Repair (TEVAR)
Endovascular Aneurysm Repair (EVAR) Endovascular stent grafts are typically used to reinforce weakened vessels or aneurysms. Typical sites are abdominal or thoracic aneurysms.
Endovascular Aneurysm Repair (EVAR) Indications for surgery: Asymptomatic patients with aneurysm >5cm Symptomatic patients Abdominal, back or groin pain Pulsatileabdominal mass
EVAR Follow up care will include: CT imaging performed at 1,3,6 and 12 months post op and yearly thereafter to evaluatefor endovascular leaks, stent migration and infection
Thoracic Endovascular Aneurysm Repair (TEVAR) Indications for surgery: Asymptomatic patients with a descending aortic aneurysm >5cm Symptomatic patients Pain in the chest, neck or back Swelling of the head, neck and arms
TEVAR Shortness of breath Difficulty swallowing Heart failure Complications are far less than those of open surgical repair.
Vascular Surgery Vascular surgery is the corrective treatment for patients with vascular insufficiency and is only indicated for symptomatic patients. It is a major operative procedure with several risks and complications: Hematoma formation Reocclusion of the vessel
Vascular Surgery Aggravation of any pre-existing medical conditions such as cardiac or kidney disease Mesenteric ischemia Abdominal compartment syndrome
Vascular bypass surgery Bypass surgery is performed in order to restore blood flow to an area of poor circulation (revascularization). Some common bypass procedures include: Aortobifemoral Femoropopliteal Femorotibial
Aortobifemoral (ABF) bypass This procedure reroutes blood from the abdominal aorta to the femoral arteries using a synthetic graft.
Femoropopliteal bypass Femoropopliteal bypass redirects blood flow to the popliteal artery above or below the knee. This is done when the patient becomes symptomatic presenting with either ulcers to the affected limb and or pain at rest which is caused by a decrease in arterial flow to the limb.
Femorotibial bypass Blood is rerouted between the femoral and tibial arteries.
Femorofemoral bypass A graft used to bypass occluded iliac arteries which has very high long-term patency rates. Preferable over aortofemoral bypass since there is no abdominal incision or aortic clamping, decreasing many post operative complications.
Abdominal Aortic Aneurysm Resection (AAAR) When the wall of the abdominal aorta becomes dilated an aneurysm develops. They typically do not require surgical repair unless they are large (> 5cm) or the patient becomes seriously symptomatic.
AAAR Surgery is performed by clamping the abdominal aorta and placing a graft to enclose the aneurysm, thus preventing leakage and/ or rupture. Triad of a ruptured abdominal aneurysm: hypotension abdominal or back pain pulsatile abdominal mass.
AAAR AAA ruptured is fatal outside of a major operative center. Surgical repair is a major procedure with several complications. Mortality rates are around 40%. Nursing management post-op will include: Frequent vital signs Peripheral perfusion checks via doppler
AAAR Continuous EKG monitoring w/ST segment monitoring Tight control of blood pressure Strict I&O to monitor kidney function Monitoring for bleeding complications
AAAR One of the latest techniques to repair aneurysms is by the use of endografts. It is less invasive than open surgery and has a lower risk of complications.
Aortoiliac Endarterectomy This procedure is less invasive than open surgery in restoring blood flow to the iliac arteries. It is ideal for younger patients who may require over their lifetime a second procedure.
Marfan’s syndrome • A connective tissue disorder. It is characterized by a generalized weakening of the cardiovascular and musculoskeletal systems. • Patients are predisposed to mitral valve prolapse and ascending aortic aneurysms.
Dissecting Aneurysm A dissection is a tear that develops in the inner layer of the aorta. As blood leaks through to the middle layer, a separation occurs between the inner layer and middle layers. Untreated it will rupture through the outer layer of the aorta, a situation which usually results in death.
Dissecting Aneurysm Type I or Type A Originates in the ascending aorta Most commonly seen in patients under 65 Most lethal form of dissection
Dissecting Aneurysm Type II Originates and is confined to the ascending aorta Commonly seen with Marfan syndrome
Dissecting Aneurysm Type III Originates in the descending aorta Most commonly seen in the elderly with atherosclerosis and untreated HTN