Download

1 / 38
430 likes | 898 Vues
Deep Vein Thrombosis. DR. SRINIVAS RAJKUMAR THIRAVIARAJ. DVT is the formation of thrombus deep veins predominantly in the legs. Also Upper Limb Paget Schrotter Syndrome – Ax V Thrombosis May Thurner Syndrome - LIV compression by RIA. contents. Importance Anatomy Pathophysiology

E N D
Deep Vein Thrombosis DR. SRINIVAS RAJKUMAR THIRAVIARAJ
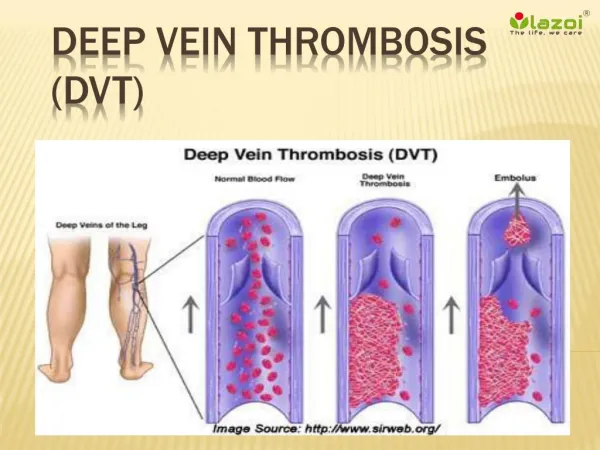
DVT is the formation of thrombus deep veins predominantly in the legs
Also • Upper Limb • Paget Schrotter Syndrome – Ax V Thrombosis • May Thurner Syndrome - LIV compression by RIA
contents • Importance • Anatomy • Pathophysiology • Risk Factors • Diagnosis • Management • Follow Up/ Complications • Prevention
Venous thromboembolism (VTE), • Deep venous thrombosis (DVT) and Pulmonary embolism (PE), One of the three major cardiovascular causes of death, along with myocardial infarction and stroke
PE – most common preventable cause of death among hospitalized patients. PE and DVT occurring after total hip or knee replacement are unacceptable "never events" and are no longer reimbursable.
The long-term effects of nonfatal VTE lower the quality of life. • Postphlebitic syndrome, which eventually occurs in more than one-half of DVT patients – No effective management possible
PATHOPHYSIOLOGY • Virchow’s Triad • Venous Stasis • Hypercoagulabilty • Endothelial Damage
ACQUIRED RISK FACTORS • Older age • Major surgery and orthopedic surgery • Cancers, especially of the bone, ovary, brain, pancreas, and lymphomas • Inactivity and immobilization, as with orthopedic casts, sitting, travel, bed rest, and hospitalization • Pregnancy and the postpartum period • Antiphospholipid syndrome • Trauma, minor leg injury, and lower limb amputation • Previous VTE
Combined oral contraceptives • Hormonal replacement therapy • Central venous catheters • Inflammatory diseases/some autoimmune diseases • Nephrotic syndrome • Obesity • Infection • HIV • Polycythemia vera • Chemotherapy • Intravenous drug use
INHERITED • Antithrombin deficiency • Protein C deficiency • Protein S deficiency (type I) • Factor V Leiden • Prothrombin G20210A • Dysfibrinogenemia • Non-O blood type
OTHERS: • Low free protein S • Activated protein C resistance • High factor VIII levels • Hyperhomocysteinemia • High fibrinogen levels • High factor IX levels • High factor XI levels
DIAGNOSIS • Clinical Examination • Only 1/4th of DVT Produces Clinical Signs & Symptoms • Most important Physical Sign – Swelling of Limbs • Muscles Become Stiff & Hard – M/I than Tenderness
Homan’s Sign – Forcible Dorsiflexion • Moses Sign – Squeezing from side to side • May Dislodge the Clot & Increase PE Risk
The sensitivity of the d-dimer is >80% for DVT (including isolated calf DVT) and >95% for PE. • With Suspected DVT, Doppler/Duplex USG should be preferred to D-Dimer
postphlebitic syndrome • A late effect of DVT -occurs in more than one-half of DVT patients. • Causes the venous valves of the leg to become incompetent and exude interstitial fluid. • Chronic ankle or calf swelling and leg aching, especially after prolonged standing. • Severe postphlebitic syndrome causes skin ulceration, especially in the medial malleolus of the leg. There is no effective medical therapy for this condition.
Patients undergoing surgery for cancer have a higher risk of postoperative deep vein thrombosis (DVT) than those having surgery for nonmalignant diseases. • Longer time to recover from Surgery & Additional Functional limitation due to cancer also increases the risk.
Tumors Strongly Associated With Thrombosis • Autopsy studies and retrospective reviews suggest that cancers of the pancreas, lung, and stomach, and adenocarcinomas of unknown primary, are most strongly associated with thrombosis, adding to the view that mucin-producing cancers are the most often associated with VTE.
Lung cancer accounted for 21% of cases • Colon cancer for 18%, and • Prostate cancer for 17%
NON PHARMACOLOGICAL MANAGEMENT • Leg Elevation • Ambulation • Fitted Graduated Compression Stockings Special Situations • IVC Filters • Embolectomy
Mini-UFH, mini-dose unfractionated heparin, 5000 units subcutaneously twice (less effective) or three times daily (more effective); LMWH, low-molecular-weight heparin, enoxaparin, 40 mg once daily, or dalteparin, 2500 or 5000 units once daily; • IPC, intermittent pneumatic compression devices.
Minimum distance of walking required daily to prevent venous thromboembolism was 398 m • Wayman Unit= 398m / 0.5 Miles
SURGICAL PROPHYLAXIS • Low Dose Prophylaxis – UFH 5000 Units Deep S.C 2hrs before 5000 Units 8-12 hrs thereafter as required
For Active Phlebitis • Medium Dose – 20,000 to 60,000 units per day For PTE High Dose-60,000 to 120,000 Units/Day
Weight Based Dosing Regimen • Initial Therapy • Bolus – 80 U/Kg • Infusion 18U/Kg/Hr • UFH
LMWH & Pentasaccharide • Enoxaparin 1mg/kg/sc q12h or 1.5mg/kg/24h • Tinzaparin 175 IU/Kg SC Daily • Dalteparin 200 Iu/Kg SC Daily • Fondaparinux 5.0 mg sc daily(50 kg) 7.5mg(50-100kg) 10 mg sc (100+kg)
To Continue Treatment ? Reversible risk factors – 3months Isolated Calf vein DVT – Serial Imaging 2 wks If Extension – Anticoagulation With Cancer, Decision to be Individualised Usually Active Cancer + DVT = 6 months Tx
It is ideal to continue OP treatment with LMWH as OD (Dalteparin 200 IU/Kg OD 1 m.o continue 150 IU/Kg for 5 months) Warfarin – INR 2.5(2-3) – Higher incidence of complications and futher VTE episodes compared to LMWH.