Download
1 / 20
210 likes | 376 Vues
Study Design for a Randomized Controlled Trial of Osmotic-Release Methylphenidate (OROS-MPH) for Attention Deficit Hyperactivity Disorder in Adolescents with Substance Use Disorders. Presenter: Theresa Winhusen, Ph.D.

E N D
Study Design for a Randomized Controlled Trial of Osmotic-Release Methylphenidate (OROS-MPH) for Attention Deficit Hyperactivity Disorder in Adolescents with Substance Use Disorders Presenter: Theresa Winhusen, Ph.D. June 14, 2006, Pharmacological Treatment of ADHD in Substance-Abusing Adolescents and Adults: New Findings, Research Directions, and Clinical Implications: 3:10 – 3:30
Principal Investigators Principal Investigator • Paula Riggs MD University of Colorado at Denver & Health Sciences Center (UCDHSC) Co-Principal Investigators • Theresa Winhusen PhD • Robert Davies MD, Medical Co LI (UCDHSC)
Background & Significance • 30-50% of adolescents in substance treatment have ADHD • ADHD associated with: • More severe substance abuse • Worse behavior problems • Poorer treatment outcomes
Background & Significance Integrated treatment is considered to be a core drug treatment principle (NIDA, 1999) Recent community treatment survey • < 50% had “dual diagnosis” programs • Of those with dual diagnosis programs: • 43.4% did not offer prescription meds • 37.8% did not offer psychiatric/psychological evaluation Motjabai, 2004
Background & Significance • One RCT targeting ADHD in adolescents with co-occurring SUD • 12 week trial pemoline* n=69, adolescents 13-19 • Similar safety, efficacy for ADHD as in adolescents without SUD • No impact on drug use in the ABSENCE of specific substance treatment Riggs et al 2004 *Schedule 1V psychostimulant
Treatment of ADHD +/- SUD Schedule II psychostimulants, gold standard • Non-scheduled alternatives-- bupropion and atomoxetine-- have lower effect sizes (.5 and .7) OROS-MPH/Concerta • Long acting (12 hours); once daily dosing • Equivalent efficacy to short acting psychostimulants • Controlled delivery system likely reduces abuse potential
Standardized SUD Treatment • Individual Manualized Cognitive Behavioral Therapy (CBT) • Found effective for SUD in adolescents • Individual, not group, due to feasibility • 16 sessions, including up to 3 family sessions
Study Objectives • Primary Objectives • 1a Evaluate safety and efficacy of OROS-MPH vs. Placebo for ADHD in adolescents with SUD • 1b Evaluate impact of treatment of ADHD with OROS-MPH on substance treatment outcomes
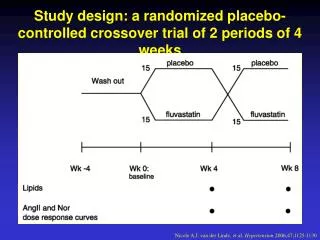
Study Design 16-week randomized controlled trial • OROS-MPH (72mg/day) vs placebo • CBT for SUD • Weekly • Outpatient Power • N= 300 to detect low/medium effect size (.4) • 11 study sites
Study Sites • Wave 1 • LRADAC, South Carolina • Synergy, Colorado • STARR, Northern New England • Wave 2 • Operation PAR, Florida • Gateway, Florida • Mountain Manor, Mid-Atlantic • Crittenton, Ohio Valley • St Lukes Roosevelt, Long Island • MHMR of Tarrant County, Texas • Rehab After Work, Delaware Valley • Addiction Medicine Services, Appalachian Tri State
Study Participants Participants • Inclusion • Adolescents (13-18) • DSM IV ADHD • At least one SUD • Exclusion • serious medical illness • bipolar • psychosis • opiate dependence • methamphetamine abuse, dependence • other treatment; psychotropics
Primary Outcome Measures • DSM-IV ADHD Symptom Checklist • Number of Use Days -Substance Use Self-Report using the TLFB
Other Efficacy Measures ADHD • Clinician Global Impression of Improvement (CGI-I) Rating Scale Substance Use Outcomes • Frequency of Drug Use (TLFB) • Urine Toxicology • Proportion of Negative Urines
Safety Measures • Vital Signs/Weight • Pregnancy Test • Adverse Events • Prior/Concomitant Medications • Lab values (urinalysis, CBC, LFTs)
Study Progress • Wave 1 Sites Initiated March 2006 • Wave 2 Site Initiation June-July 2006
Study Timeline & Enrollment Schedule 2006 A/4 M/5 J/6 J/7 A/8 S/9 O/10 N/11 D/12 6 12 18 21 43 65 87 109 131 2007 J/1 F/2 M/3 A/4 M/5 J/6 J/7 A/8 153 175 197 219 241 263 285 307 S/9 O/10 N/11 D/12 2008 J/1F/2 M/3 A/4 Initial projection enrollment completion midpoint enrollment completed 16 wk study completion F/u study completion Study close out, data lock, manuscript preparation