Download
1 / 1
10 likes | 173 Vues
Expanding DOTS? Time for cost-effective diagnostic strategies for the poorest in Malawi. Mann G 1 , Squire SB 2, , Nhlema B 3 , Luhanga T 4 , Salaniponi FML 5 , Kemp J 2,3. AIM To assess possible alternative cost-effective strategies for TB diagnosis for the poorest. OBJECTIVES

E N D
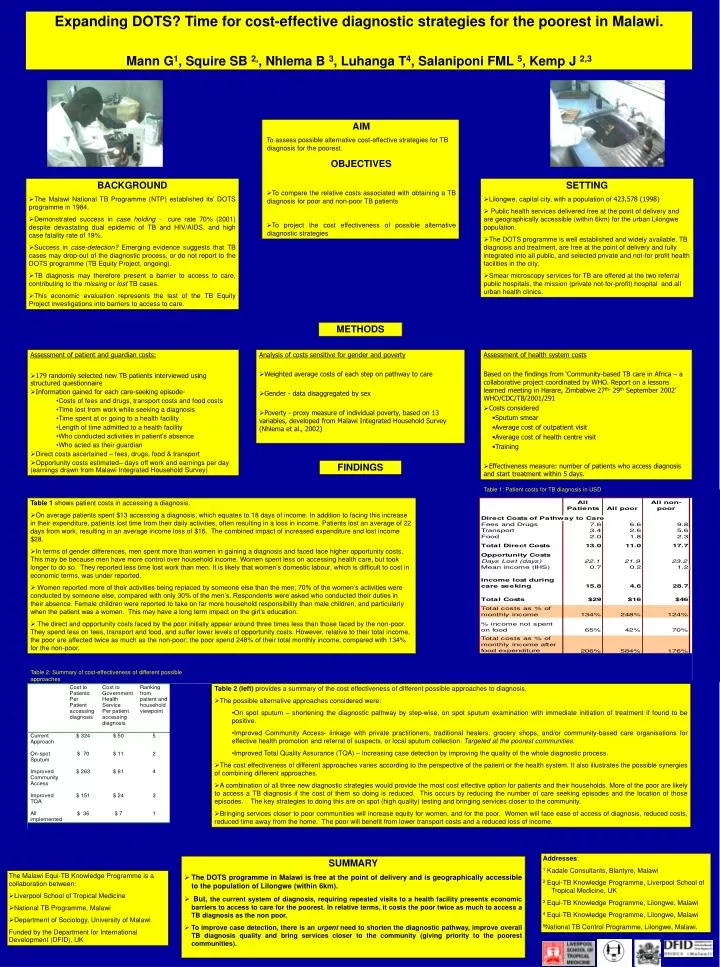
Expanding DOTS? Time for cost-effective diagnostic strategies for the poorest in Malawi. Mann G1, Squire SB 2,, Nhlema B 3, Luhanga T4, Salaniponi FML 5, Kemp J 2,3 • AIM • To assess possible alternative cost-effective strategies for TB diagnosis for the poorest. • OBJECTIVES • To compare the relative costs associated with obtaining a TB diagnosis for poor and non-poor TB patients • To project the cost effectiveness of possible alternative diagnostic strategies • BACKGROUND • The Malawi National TB Programme (NTP) established its’ DOTS programme in 1984. • Demonstrated success in case holding - cure rate 70% (2001) despite devastating dual epidemic of TB and HIV/AIDS, and high case fatality rate of 19%. • Success in case-detection? Emerging evidence suggests that TB cases may drop-out of the diagnostic process, or do not report to the DOTS programme (TB Equity Project, ongoing). • TB diagnosis may therefore present a barrier to access to care, contributing to the missing or lost TB cases. • This economic evaluation represents the last of the TB Equity Project investigations into barriers to access to care. • SETTING • Lilongwe, capital city, with a population of 423,578 (1998) • Public health services delivered free at the point of delivery and are geographically accessible (within 6km) for the urban Lilongwe population. • The DOTS programme is well established and widely available. TB diagnosis and treatment, are free at the point of delivery and fully integrated into all public, and selected private and not-for profit health facilities in the city. • Smear microscopy services for TB are offered at the two referral public hospitals, the mission (private not-for-profit) hospital and all urban health clinics. METHODS • Assessment of patient and guardian costs: • 179 randomly selected new TB patients interviewed using structured questionnaire • Information gained for each care-seeking episode- • Costs of fees and drugs, transport costs and food costs • Time lost from work while seeking a diagnosis • Time spent at or going to a health facility • Length of time admitted to a health facility • Who conducted activities in patient’s absence • Who acted as their guardian • Direct costs ascertained – fees, drugs, food & transport • Opportunity costs estimated– days off work and earnings per day (earnings drawn from Malawi Integrated Household Survey) • Analysis of costs sensitive for gender and poverty • Weighted average costs of each step on pathway to care • Gender - data disaggregated by sex • Poverty - proxy measure of individual poverty, based on 13 variables, developed from Malawi Integrated Household Survey (Nhlema et al., 2002) Assessment of health system costs Based on the findings from ‘Community-based TB care in Africa – a collaborative project coordinated by WHO. Report on a lessons learned meeting in Harare, Zimbabwe 27th- 29th September 2002’ WHO/CDC/TB/2001/291 • Costs considered • Sputum smear • Average cost of outpatient visit • Average cost of health centre visit • Training • Effectiveness measure: number of patients who access diagnosis and start treatment within 5 days. FINDINGS Table 1: Patient costs for TB diagnosis in USD • Table 1 shows patient costs in accessing a diagnosis. • On average patients spent $13 accessing a diagnosis, which equates to 18 days of income. In addition to facing this increase in their expenditure, patients lost time from their daily activities, often resulting in a loss in income. Patients lost an average of 22 days from work, resulting in an average income loss of $16. The combined impact of increased expenditure and lost income $28. • In terms of gender differences, men spent more than women in gaining a diagnosis and faced face higher opportunity costs. This may be because men have more control over household income. Women spent less on accessing health care, but took longer to do so. They reported less time lost work than men. It is likely that women’s domestic labour, which is difficult to cost in economic terms, was under reported. • Women reported more of their activities being replaced by someone else than the men; 70% of the women’s activities were conducted by someone else, compared with only 30% of the men’s. Respondents were asked who conducted their duties in their absence. Female children were reported to take on far more household responsibility than male children, and particularly when the patient was a women. This may have a long term impact on the girl’s education. • The direct and opportunity costs faced by the poor initially appear around three times less than those faced by the non-poor. They spend less on fees, transport and food, and suffer lower levels of opportunity costs. However, relative to their total income, the poor are affected twice as much as the non-poor; the poor spend 248% of their total monthly income, compared with 134% for the non-poor. Table 2: Summary of cost-effectiveness of different possible approaches • Table 2 (left) provides a summary of the cost effectiveness of different possible approaches to diagnosis. • The possible alternative approaches considered were: • On spot sputum – shortening the diagnostic pathway by step-wise, on spot sputum examination with immediate initiation of treatment if found to be positive. • Improved Community Access- linkage with private practitioners, traditional healers, grocery shops, and/or community-based care organisations for effective health promotion and referral of suspects, or local sputum collection. Targeted at the poorest communities. • Improved Total Quality Assurance (TQA) – Increasing case detection by improving the quality of the whole diagnostic process. • The cost effectiveness of different approaches varies according to the perspective of the patient or the health system. It also illustrates the possible synergies of combining different approaches. • A combination of all three new diagnostic strategies would provide the most cost effective option for patients and their households. More of the poor are likely to access a TB diagnosis if the cost of them so doing is reduced. This occurs by reducing the number of care seeking episodes and the location of those episodes. The key strategies to doing this are on spot (high quality) testing and bringing services closer to the community. • Bringing services closer to poor communities will increase equity for women, and for the poor. Women will face ease of access of diagnosis, reduced costs, reduced time away from the home. The poor will benefit from lower transport costs and a reduced loss of income. Addresses: 1 Kadale Consultants, Blantyre, Malawi 2 Equi-TB Knowledge Programme, Liverpool School of Tropical Medicine, UK 3 Equi-TB Knowledge Programme, Lilongwe, Malawi 4 Equi-TB Knowledge Programme, Lilongwe, Malawi 5National TB Control Programme, Lilongwe, Malawi. • SUMMARY • The DOTS programme in Malawi is free at the point of delivery and is geographically accessible to the population of Lilongwe (within 6km). • But, the current system of diagnosis, requiring repeated visits to a health facility presents economic barriers to access to care for the poorest. In relative terms, it costs the poor twice as much to access a TB diagnosis as the non poor. • To improve case detection, there is an urgent need to shorten the diagnostic pathway, improve overall TB diagnosis quality and bring services closer to the community (giving priority to the poorest communities). • The Malawi Equi-TB Knowledge Programme is a collaboration between: • Liverpool School of Tropical Medicine • National TB Programme, Malawi • Department of Sociology, University of Malawi • Funded by the Department for International Development (DFID), UK