Download
1 / 23
230 likes | 369 Vues
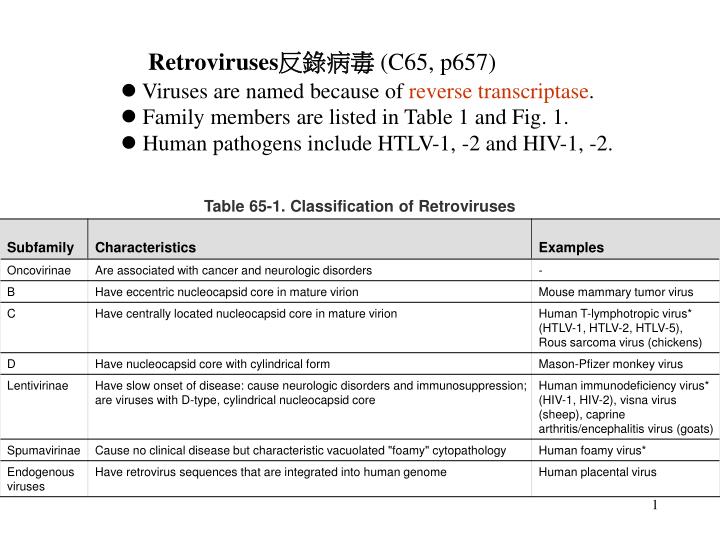
Retroviruses 反錄病毒 (C65, p657) l Viruses are named because of reverse transcriptase . l Family members are listed in Table 1 and Fig. 1. l Human pathogens include HTLV-1, -2 and HIV-1, -2. 1. Structure: +ssRNA (about 9 kb for HIV) X2, capsid and envelope) (Fig. 3).

E N D
Retroviruses反錄病毒 (C65, p657) lViruses are named because of reverse transcriptase. lFamily members are listed in Table 1 and Fig. 1. lHuman pathogens include HTLV-1, -2 and HIV-1, -2.
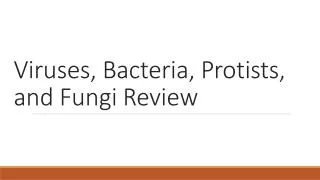
1.Structure: +ssRNA (about 9 kb for HIV) X2, capsid and envelope) (Fig. 3) 2. viral genome include LTR, Gag(group specific Ag, capsid, matrix, and nucleic acid proteins), pol (reverse transcriptase, integrase, polymerase, and protease), and env (envelope glycoproteins).
﹛ pol Simple v.s. complex viruses
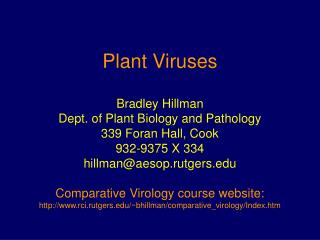
2.Replication (Fig. 5) -- Virus infects mφ, dendritic cells, microglial cells and activated T cells via CD4 and CCR5 ( M-tropic) and naïve and helper T cells via CD4 and CXCR4 (T-tropic)(Fig. 6 ).
Drug target • Provirus • Error rate (about • 1/2,000 base)
4.Human immunodeficiency virus (HIV) -- It is non-oncogenic virus. -- HIV infects CD4-expressing mφand T cells (M-tropic T-tropic). -- Infection reduces the number (due to cytolysis by virus or cytotoxic T cells) and function of CD4 T cells to cause acquired immunodeficiency syndrome (AIDS).
l Epidemiology: a. Based on the estimation in 2003, there are 5 million new cases each year and 3 million death per year. b. Geographical distribution: HIV-1 is in Africa, Asia, and US. HIV-2 is in Africa. c. Global distribution (Fig. 12) 4-7
d. Transmission: HIV is transmitted by body fluid such as blood, semen, and vaginal secretion (Fig. 11 and Table 4). e. High risk population includes: sexually active people, drug abusers, people receiving blood, blood product, and organs before 1985, and health care workers.
Clinical Symptoms: --acute infection: flu like symptoms, mononucleosis, and aseptic meningitis --Stage 1: lymphoadenopathy --Stage 2: weight loss, malaise, opportunist infections, diarrhea, night sweats, fatigue, and wasting (slim) disease in African --Stage 3 (Onset of disease occurs when CD4 T cells are < 200/μl blood) Full blown AIDS with weight loss, diarrhea for > 1 month, and indicator diseases (p. 668, Table 5) . 14
16 BOX 65-4. Potential Antiviral Therapies for HIV Infection • Nucleoside Analogue Reverse Transcriptase Inhibitors • Azidothymidine (AZT) (Zidovudine/retrovir) • Dideoxycytidine (ddC) (Zalcitabine ) • Dideoxyinosine (ddI) (Didanosine ) • d4T (Stavudine ) • 3TC (Lamivudine ) • Tenofovir disoproxil fumarate (adenosine class) (Viread) • ABC (Abacavir) • Non-nucleoside Reverse Transcriptase Inhibitors • Nevirapine (Viramune) • Delavirdine (Rescriptor) • Efavirenz (Sustiva) • Protease Inhibitors • Saquinavir (Invirase/Fortovase) • Ritonavir (Norvir) • Indinavir (Crixivan) • Lopinavir (Kaletra) • Nelfinavir (Viracept) • Amprenavir (Agenerase) • Fosamprevavir (Lexavir) • Atazanavir (Reyataz) • Fusion Inhibitor • T-20 (enfuvirtide/Fuzeon) • Highly Active Antiretroviral Therapy (HAART) (Combination) • Abacavir/zidovudine/lamivudine (Trizivir) • Indinavir/AZT/3TC • Ritonavir/AZT/3TC • Nelfinavir/AZT/3TC • Nevirapine/AZT/ddI • Nevirapine/indinavir/3T R10 lPrevention, treatment, and control a. Four types of drugs b. AZT is for infected pregnant women. c. Antiviral drug cocktail (highly active antiretroviral treatment, HARRT) is used for infected people. d. Education: monogamous and safe sex; use of condoms; promotion of clean needles for drug abusers (needle exchange) e. Blood, blood product, and organ screening f. Infection control in the hospitals c.There is no effective preventive or therapeutic vaccine because HIV mutates rapidly, there is no good vaccine strategy, and animal model is not available.
17 2. Oncogenic retroviruses cause leukemia, sarcoma, and lymphoma. They are not cytolytic and belonged to Oncovirinae (also called RNA tumor viruses). l Sarcoma, lymphoma, and acute leukemia (non human) viruses have incorporated cellular genes (protooncogenes) encoding growth-controlling factors. . l Representatives of viral oncogenes are listed in Table 8. 4-11
l Human pathogens include HTLV-1, 2, and 5 a. HTLV-1 causes adult acute T-cell lymphocytic leukemia (ATLL) and HTLV-1-associated myelopathy (an neurological disorder) HTLV-2 is isolated from atypical form hairy cell leukemia, and HTLV-5 is isolated from malignant cutaneous lymphoama.
b. They can not transform cells so they induce disease by different mechanisms. Table 65-7. Mechanisms of Retrovirus Oncogenesis 19
b. Pathogenesis and immunity l Virus is transmitted by sexual intercourse and body fluid like blood and breast milk. l Virus infects CD4 T cells (which reside in skin) and neurons. l Viral gene, tax, induces IL-2 and its receptor to cause clonal outgrowth of particular T-cells in adult ATLL in about 30 years. l Infected hosts elicit Ab against virus glycoprotein gp46. l Virus infection causes immunosuppression. c. Epidemiology. l HTLV-1 is transmitted by the same route as HIV. l It is endemic in some areas. (35% people are infected in Okinawa). In those areas, children acquire virus in breast milk and adults are infected sexually. Intravenous drug abuse and blood transfusion also transmit virus in US.
d. Clinical syndromes l ATLL develops in 5% infected patients over a 30- to 50-year period. Malignant CD4 helper cells are pleomorphic and have lobulated nuclei (like flowers). l Skin lesions develop in ATLL patients. l ATTL patients die within a year of diagnosis. 21
e.Lab. Diagnosis ELISA is used to detect viral antigens and specific Ab, and RT-PCR is used to detect viral genome. f.Treatment, prevention and control. lAZT plus interferon alpha are used to treat ATTL. No treatment and vaccine are available for virus infection. Control measures are similar to HIV.
A 28-year-old man had several complaints. He had a bad case of thrush (oral candidiasis) and low-grade fever, had serious bouts of diarrhea, had lost 20 pounds in the past year without dieting, and, most seriously, complained of difficulty breathing. His lungs showed a bilateral infiltrate on radiographic examination, characteristic of P. carinii pneumonia. A stool sample was positive for Giardia organisms. He was a heroin addict and admitted to sharing needles at a "shooting gallery." • What laboratory tests should have been done to support and confirm a diagnosis of HIV infection and AIDS? • How did this man acquire the HIV infection? What are other high-risk behaviors for HIV infection? • What was the immunologic basis for the increased susceptibility of this patient to opportunistic infections? • What precautions should have been taken in handling samples from this patient? • Several forms of HIV vaccines are being developed. What are possible components of an HIV vaccine? Who would be appropriate recipients of an HIV vaccine?