Download
1 / 1
10 likes | 89 Vues
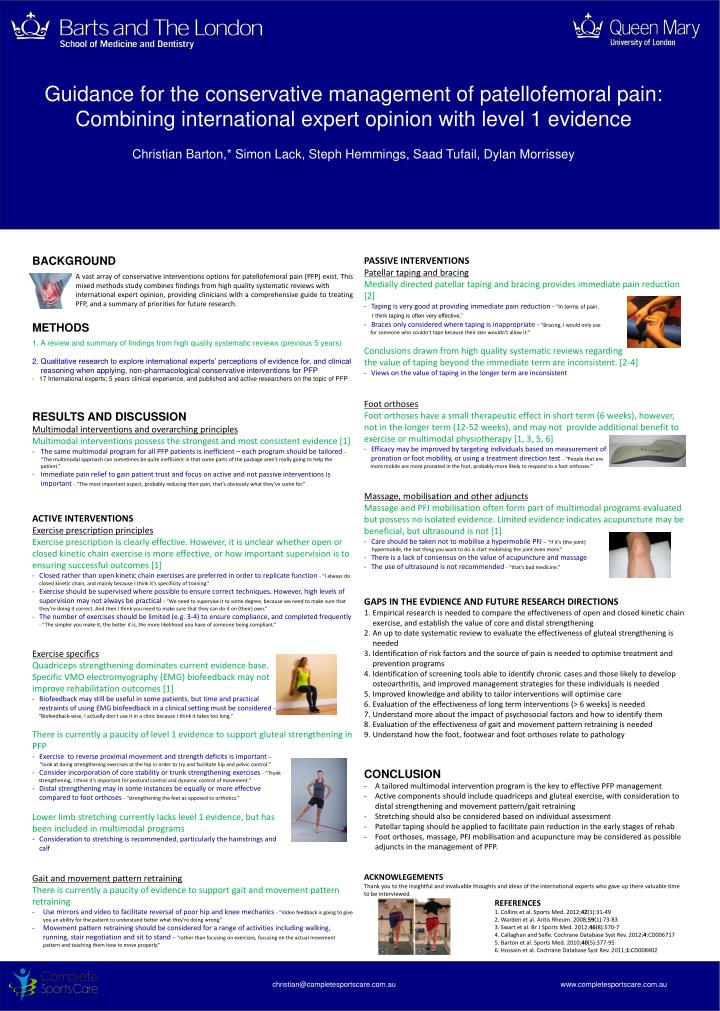
Guidance for the conservative management of patellofemoral pain: Combining international expert opinion with level 1 evidence Christian Barton,* Simon Lack, Steph Hemmings , Saad Tufail , Dylan Morrissey. BACKGROUND

E N D
Guidance for the conservative management of patellofemoral pain: Combining international expert opinion with level 1 evidence Christian Barton,* Simon Lack, StephHemmings, SaadTufail, Dylan Morrissey • BACKGROUND • A vast array of conservative interventions options for patellofemoral pain (PFP) exist. This mixed methods study combines findings from high quality systematic reviews with international expert opinion, providing clinicians with a comprehensive guide to treating PFP, and a summary of priorities for future research. • METHODS • A review and summary of findings from high quality systematic reviews (previous 5 years) • Qualitative research to explore international experts’ perceptions of evidence for, and clinical reasoning when applying, non-pharmacological conservative interventions for PFP • 17 International experts; 5 years clinical experience, and published and active researchers on the topic of PFP • RESULTS AND DISCUSSION • Multimodal interventions and overarching principles • Multimodal interventions possess the strongest and most consistent evidence [1] • The same multimodal program for all PFP patients is inefficient – each program should be tailored - “The multimodal approach can sometimes be quite inefficient in that some parts of the package aren’t really going to help the patient.” • Immediate pain relief to gain patient trust and focus on active and not passive interventions is important - “The most important aspect, probably reducing their pain, that’s obviously what they’ve come for.” • ACTIVE INTERVENTIONS • Exercise prescription principles • Exercise prescription is clearly effective. However, it is unclear whether open or closed kinetic chain exercise is more effective, or how important supervision is to ensuring successful outcomes [1] • Closed rather than open kinetic chain exercises are preferred in order to replicate function - “I always do closed kinetic chain, and mainly because I think it’s specificity of training.” • Exercise should be supervised where possible to ensure correct techniques. However, high levels of supervision may not always be practical - “We need to supervise it to some degree, because we need to make sure that they’re doing it correct. And then I think you need to make sure that they can do it on (their) own.” • The number of exercises should be limited (e.g. 3-4) to ensure compliance, and completed frequently - “The simpler you make it, the better it is, the more likelihood you have of someone being compliant.” • Exercise specifics • Quadriceps strengthening dominates current evidence base. • Specific VMO electromyography (EMG) biofeedback may not • improve rehabilitation outcomes [1] • Biofeedback may still be useful in some patients, but time and practical • restraints of using EMG biofeedback in a clinical setting must be considered – • “Biofeedback-wise, I actually don’t use it in a clinic because I think it takes too long.” • There is currently a paucity of level 1 evidence to support gluteal strengthening in PFP • Exercise to reverse proximal movement and strength deficits is important – • “Iookat doing strengthening exercises at the hip in order to try and facilitate hip and pelvic control.” • Consider incorporation of core stability or trunk strengthening exercises - “Trunk • strengthening, I think it’s important for postural control and dynamic control of movement.” • Distal strengthening may in some instances be equally or more effective • compared to foot orthoses- “strengthening the feet as opposed to orthotics.” • Lower limb stretching currently lacks level 1 evidence, but has • been included in multimodal programs • Consideration to stretching is recommended, particularly the hamstrings and • calf • Gait and movement pattern retraining • There is currently a paucity of evidence to support gait and movement pattern retraining • Use mirrors and video to facilitate reversal of poor hip and knee mechanics - “Video feedback is going to give you an ability for the patient to understand better what they’re doing wrong.” • Movement pattern retraining should be considered for a range of activities including walking, running, stair negotiation and sit to stand – “rather than focusing on exercises, focusing on the actual movement pattern and teaching them how to move properly.” • PASSIVE INTERVENTIONS • Patellar taping and bracing • Medially directed patellar taping and bracing provides immediate pain reduction [2] • Taping is very good at providing immediate pain reduction - “In terms of pain, • I think taping is often very effective.” • Braces only considered where taping is inappropriate - “Bracing, I would only use • for someone who couldn’t tape because their skin wouldn’t allow it.” • Conclusions drawn from high quality systematic reviews regarding • the value of taping beyond the immediate term are inconsistent. [2-4] • Views on the value of taping in the longer term are inconsistent • Foot orthoses • Foot orthoses have a small therapeutic effect in short term (6 weeks), however, not in the longer term (12-52 weeks), and may not provide additional benefit to exercise or multimodal physiotherapy [1, 3, 5, 6] • Efficacy may be improved by targeting individuals based on measurement of • pronation or foot mobility, or using a treatment direction test - “People that are • more mobile are more pronated in the foot, probably more likely to respond to a foot orthoses.” • Massage, mobilisation and other adjuncts • Massage and PFJ mobilisation often form part of multimodal programs evaluated but possess no isolated evidence. Limited evidence indicates acupuncture may be beneficial, but ultrasound is not [1] • Care should be taken not to mobilise a hypermobile PFJ – “If it’s (the joint) • hypermobile, the last thing you want to do is start mobilising the joint even more.” • There is a lack of consensus on the value of acupuncture and massage • The use of ultrasound is not recommended - “that’s bad medicine.” • GAPS IN THE EVDIENCE AND FUTURE RESEARCH DIRECTIONS • Empirical research is needed to compare the effectiveness of open and closed kinetic chain exercise, and establish the value of core and distal strengthening • An up to date systematic review to evaluate the effectiveness of gluteal strengthening is needed • Identification of risk factors and the source of pain is needed to optimise treatment and prevention programs • Identification of screening tools able to identify chronic cases and those likely to develop osteoarthritis, and improved management strategies for these individuals is needed • Improved knowledge and ability to tailor interventions will optimise care • Evaluation of the effectiveness of long term interventions (> 6 weeks) is needed • Understand more about the impact of psychosocial factors and how to identify them • Evaluation of the effectiveness of gait and movement pattern retraining is needed • Understand how the foot, footwear and foot orthoses relate to pathology • CONCLUSION • A tailored multimodal intervention program is the key to effective PFP management • Active components should include quadriceps and gluteal exercise, with consideration to distal strengthening and movement pattern/gait retraining • Stretching should also be considered based on individual assessment • Patellar taping should be applied to facilitate pain reduction in the early stages of rehab • Foot orthoses, massage, PFJ mobilisation and acupuncture may be considered as possible adjuncts in the management of PFP. • ACKNOWLEGEMENTS • Thank you to the insightful and invaluable thoughts and ideas of the international experts who gave up there valuable time to be interviewed. • REFERENCES • 1. Collins et al. Sports Med. 2012;42(1):31-49 • 2. Warden et al. Aritis Rheum. 2008;59(1):73-83 • 3. Swart et al. Br J Sports Med. 2012;46(8):570-7 • 4. Callaghan and Selfe. Cochrane Database Syst Rev. 2012;4:CD006717 • 5. Barton et al. Sports Med. 2010;40(5):377-95 • 6. Hossain et al. Cochrane Database Syst Rev. 2011;1:CD008402 christian@completesportscare.com.au www.completesportscare.com.au christian@completesportscare.com.au www.completesportscare.com.au