Download
1 / 69
890 likes | 2.54k Vues
Leishmaniasis. Different stages of Haemoflagellates. Leishmania life cycle. Promastigote Amasitgote Transformation. Leishmania life cycle. Amastigotes replicate in reticuloendothelial cells (mononuclear cells) including; Monocytes Macrophages in lymph nodes, spleen, and lung;

E N D
Leishmania life cycle PromastigoteAmasitgote Transformation
Leishmania life cycle • Amastigotes replicate in reticuloendothelial cells (mononuclear cells) including; • Monocytes • Macrophages in lymph nodes, spleen, and lung; • Kupffer cells in sinusoids of liver • Microglial cells in the central nervous system. • Dendriticcells Promastigotes reproduce in biting fly (Phlebotomus, Lutzomyia)
Leishmania infects and thrives in macrophages • Promastigotes attached to CR1 and CR3 receptors on the macrophages • The parasite invades its host cell passively by phagocytosis (parasitophorous vacuole)
Leishmania sp. amastigote stage • Ovoid smallintracellular parasites in a bone marrow aspirate. The typical rod shaped kinetoplast is seen besides the nucleus.(Giemsa stain).
Leishmaniasis vectors • There are over 600 species of sand flies divided into five genera. More than 30 species are proved vectors. • Phlebotomus in the Old-world and Lutzomia in the New world are vectors of human leishmaniasis.
Procyclics and Metacyclic Promastigotes • Amastigotes are released by digestion, transform into procyclic promastigotes and attach to the midgut epithelium • Attached promastigotes divide rapidly • Metacyclic (infective) promastigotescease replication, detach and pass forward into the pharynx from where they are regurgitated into the bite site (detached) (attached)
Two subgenera of Leishmania genus • subgenus Leishmania: develops in the sand fly’s midgut and foregut (suprapylorian) • Both Old world and New world visceral and cutaneous species • subgenus Viannia: develops in the hindgut and midgut (peripylarian). • L.braziliensis complex, L.guyanensis complex.
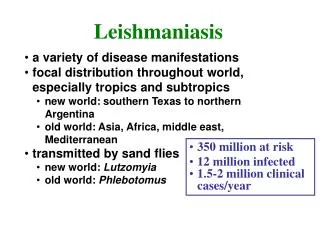
Importance • Leishmaniasis is a parasitic disease transmitted by the bite of sand flies. • In at least 88 countries. • 350 million people at risk. • 12 million people are affected by leishmaniasis. • 1.5-2 million new cases of cutaneous leishmaniasis estimated to occur annually. • 500 000 new cases of VL which occur annually. • 90% of CL cases were from Afghanistan, Algeria, Brazil, Iran, Peru, Saudi Arabia and Syria. • 90% of VL cases were from Bangladesh, India, Nepal, Sudan and Brazil. • 90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru.
The disease main forms • Cutaneous leishmaniasis (CL) • 2. Visceral leishmaniasis (VL),(kala-azar) is the most severe form of the disease. Mortality rate 75-95% • 3. Mucocutaneous leishmaniasis (MCL),or espundia, disfiguring, destruction of mucous membranes of the nose, mouth and throat cavities. Reconstructive surgery of deformities is an important part of therapy
Cutaneous Leishmaniasis Skin ulcers on the exposed parts of the body such as the face, arms and legs. Old World: L. major, L. tropica, L. aethiopica (DCL) New World: L. mexicana, L. pifanoi, L. amazonensis, L. venezuelensis, L. granhami,
Cutaneous Leishmaniasis • Characterized by one or more papules, nodules and sores on the skin • Sore like a volcano with a raised edge and central crater. • Two figures including urban (dry) and rural (wet) forms. • Sores are usually painless but can become painful if secondarily infected • chronic but self-limiting
Infection remains restricted to the initial site of infection (the bite site)
Leishmania tropica • Anthroponotic Cutaneous Leishmaniasis (ACL) • Definitive Host: Humans • (occasionally dog?) • Intermediate Host: Phlebotomus sand flies • Main vector and also in Iran: P. Sergenti • Dry or urban C.L. • Face> hand, leg and… • Incubation period: 2-8 months(usually 2-3 months) • Lesion persist for several months (more than one year) then person is immune
Leishmania tropica • Sores don’t heal very quickly • Often mistaken for leprosy or tuberculosis • First sign: small papule nodule dry sore • Itching • Scar (if not treated)
Rarely can cause visceral (viscerotropic) and diffuse cutaneous infections.
Leishmania major • Wet or rural form • Definitive Host: rodents (Rodentia: Gerbillidae) as reservoir host, Humans • In Iran: Rhombomysopimus, Merioneslibycus, M.hurrianae, Tateraindica • Zoonotic Cutaneous leishmaniasis (ZCL) • Intermediate Host:Phlebotomus sand flies. In Iran: P. papatasi. • Incubation period: some weeks to 3 months ( usually 2 weeks) • First sign: small papule nodule Wet sore (exudates) • Itching • Scar (if not treated) • Disease period is usually short (2-8 months) • More in hands and feet
Sporotrichoid form Diffuse cutaneous leishmaniasis Recidivans leishmaniasis
Leprosy • It is primarily a granulomatous disease of the peripheral nerves and mucosa of the upper respiratory tract. • Skin lesions are the primary external sign. • Left untreated, leprosy can be progressive, causing permanent damage to the skin, nerves, limbs and eyes.
Lupus volgaris (a sort of cutaneus TB) • Persistent and progressive form of cutaneous TB. • Small sharply defined reddish-brown lesions with a gelatinous consistency (called apple-jelly nodules). • Lesions persist for years, leading to disfigurement and sometimes skin cancer
New World cutaneous leishmaniasis • L. mexicana (Chicleros Ulcer) • External ear • L. pifanoi • L. amazonensis • main cause of DCL • All four leishmaniasis forms • L. (V.) peruviana(Uta) • L. granhami • L. venezuelensis
Systemic infection of reticulo-entdothelial cells (mostly macrophages) throughout multiple internal organs and the blood
Kala-azar , Visceral Leishmaniasis • L. donovanicomplex • L. donovani(Asia, East Africa) • Strain archibaldi • L. infantum (Medditeranian basin and Middle East, in children) • L. chagasi( South & Central America) • L. tropica (viscerotropic) • L. amazonensis • Weeks to months (2-6 months) incubation period
L. donovani, anthroponotic L. infantum, zoonosis, L. donovani ,(archibaldi), zoonosis, L. chagasi, zoonotic
The most sever leishmaniasis form • Mortality of untreated disease 75-95% • Prolonged fever (usually dromedary but also continuous, reminant, interminnent) • Splenomegaly, hepatomeglay, • Weight loss (cachexia), • Progressive anemia, pancytopenia, • Hypergammaglobulinemia and hypoalbominemia • Skin darkness ( around mounth, forehead, temple) • Lymphadenopathy may be present • Elevated liver enzymes, Nausea, vomiting. • Pancytopenia: normochrome & normocytic anemia, trombocytopenia, but lymphocytosis
Visceral Leishmaniasis • Visceral leishmaniasis should be considered in every case with chronic fever returning from an endemic area. • Malaria, tropical splenomegaly, schistosomiasis, cirrhosis, portal hypertension, trypanosomiasis, milliary tuberculosis, brucellosis, typhoid fever, bacterial endocarditis, histoplasmosis, malnutrition, lymphoma, and leukemia (Singh, 2006). • Apart from fly biting, other routes including; Placental, blood transfusion, mechanical, sexual routes.
Viscerotropic leishmaniasis • L. tropica • Oligoparasitic leishmaniasis • Fever, fatigue, digestive tract problems • First in desert storm operation in Iraq among American soldiers • In Iran: One case from AIDS patient (Tehran), other case (Shiraz)
Epidemiology of visceral leishmaniasis in Iran Mediterranean Kala-azar: - Causative agent is L. infantum - Reservior host: involving canine such as Dog, Jackal, fox, wolf and other wild carnivorouses. - The probable main vector in Iran is Phlebotomus major (Fars), other vectors are P.keshishiani (Fars), P. Perfiliewi (Dashte-Moghan),P. kandelakii (Meshkinshahr). - Age distribution: the disease mainly occurs in children from 1 to 4 years of age.
Immunity • TH1: • Macrophage produces IL12 • IL12 promote TH0 to TH1 • TH1 produces INF gama, IL2, TNF • Healing and resistance to disease • TH2: • TH2 produces IL4, IL5, IL6, IL10, IL13 • Sensitivity to disease
1. Clinical Diagnosis: • Patient history ( endemic region or travel), • Signs & symptoms • Sores that will not heal, have to be referred for evaluation. • Individuals with fevers, weight loss, gastrointestinal complaints, anemia, hypergammaglobulinemia, abnormal liver tests should be referred for evaluation
Laboratory Diagnosis of leishmaniasis : 1. Cutaneous Leishmaniasis • Tissue sample (scraping, aspirate or punch biopsy) for smear and culture • Take scrapings from the sore, put on slides, stain with Wright’s or Giemsa’s stains, and look for amastigotes. • Culture (NNN & LIT, Evans, RPMI 1640), • Laboratory animals inoculation (SouriandBalb/c mouse) only for L. major (no growth in L. tropica)
Cutaneous Leishmaniasis (con.) • Leishmania skin test (Montenegro test) • 0.1 ml (1,000,000 killed L. majorpromastigote), intradermal, • 5mm< induration after 48-72h, DTH • Isoenzymeprofiles - Zymodemes • No serological approaches usually but monoclonal antibodies can be used. • DNA hybridisation - PCR
2. Visceral Leishmaniasis • Finding Leishmaniaon biopsy of bone marrow (iliac, sternum, tibia (54-86% sensitivity)), liver (60%), enlarged lymph node (64%), or spleen (98%). • Culture (NNN, Evans, LIT) • Laboratory animals IP inoculation (Golden hamester) • No LST for VL and PKDL diagnosis (Yes for VL and CL epidemiology and MCL and Lupoid diagnosis)
Visceral Leishmaniasis (con.) • Serologic tests: • Antibody detection: DAT (sen 91-100%, spe 72-95%) IFA (sen 55-70, spe 70-89) ELISA,( sen 80-100% spe 84-95) Dipstick test (rk39, recombinant antigen 39kd, sen 67-100% spe 88-100%) • DAT is easy, inexpensive, and with high specificity and sensitivity (most usage in Iran) • Antigen detection: KAtex (5-20 kd glycoprotein, membranous antigen, easy, field applicable, sen 68-100%, spe 100%, positive only in acute disease, useful for HIV/VL ) • Formel gel, (Based on hyperimmunoglobulinemia) • Multiple myeloma, Schistosomiasis • Isoenzyme profiles - Zymodemes • Monoclonal antibodies • DNA hybridisation – PCR (Schizodem)