Download
1 / 1
10 likes | 106 Vues
Since its inception by Billroth the loop gastro-jejunostomy (Billroth II) has been in continuous use to this day for over a hundred years by general, trauma and oncologic surgeons around the world.

E N D
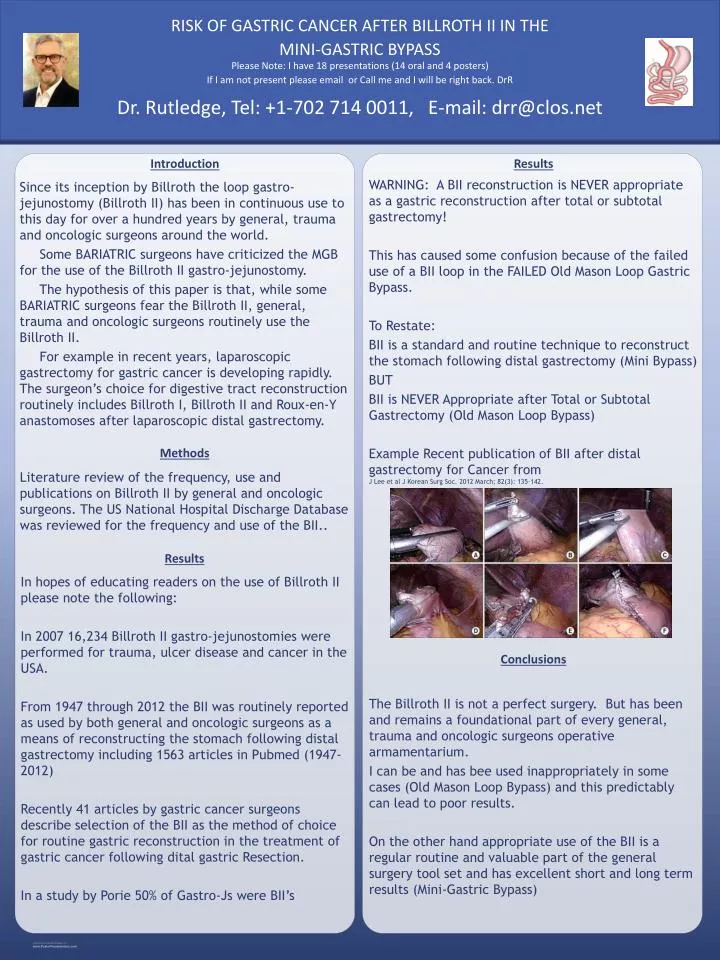
Since its inception by Billroth the loop gastro-jejunostomy (Billroth II) has been in continuous use to this day for over a hundred years by general, trauma and oncologic surgeons around the world. Some BARIATRIC surgeons have criticized the MGB for the use of the Billroth II gastro-jejunostomy. The hypothesis of this paper is that, while some BARIATRIC surgeons fear the Billroth II, general, trauma and oncologic surgeons routinely use the Billroth II. For example in recent years, laparoscopic gastrectomy for gastric cancer is developing rapidly. The surgeon’s choice for digestive tract reconstruction routinely includes Billroth I, Billroth II and Roux-en-Y anastomoses after laparoscopic distal gastrectomy. Introduction Methods Results WARNING: A BII reconstruction is NEVER appropriate as a gastric reconstruction after total or subtotal gastrectomy! This has caused some confusion because of the failed use of a BII loop in the FAILED Old Mason Loop Gastric Bypass. To Restate: BII is a standard and routine technique to reconstruct the stomach following distal gastrectomy (Mini Bypass) BUT BII is NEVER Appropriate after Total or Subtotal Gastrectomy (Old Mason Loop Bypass) Example Recent publication of BII after distal gastrectomy for Cancer from J Lee et al J Korean Surg Soc. 2012 March; 82(3): 135–142. Conclusions The Billroth II is not a perfect surgery. But has been and remains a foundational part of every general, trauma and oncologic surgeons operative armamentarium. I can be and has bee used inappropriately in some cases (Old Mason Loop Bypass) and this predictably can lead to poor results. On the other hand appropriate use of the BII is a regular routine and valuable part of the general surgery tool set and has excellent short and long term results (Mini-Gastric Bypass) Literature review of the frequency, use and publications on Billroth II by general and oncologic surgeons. The US National Hospital Discharge Database was reviewed for the frequency and use of the BII.. Dr. Rutledge, Tel: +1-702 714 0011, E-mail: drr@clos.net Please Note: I have 18 presentations (14 oral and 4 posters) If I am not present please email or Call me and I will be right back. DrR RISK OF GASTRIC CANCER AFTER BILLROTH II IN THE MINI-GASTRIC BYPASS Results In hopes of educating readers on the use of Billroth II please note the following: In 2007 16,234 Billroth II gastro-jejunostomies were performed for trauma, ulcer disease and cancer in the USA. From 1947 through 2012 the BII was routinely reported as used by both general and oncologic surgeons as a means of reconstructing the stomach following distal gastrectomy including 1563 articles in Pubmed (1947-2012) Recently 41 articles by gastric cancer surgeons describe selection of the BII as the method of choice for routine gastric reconstruction in the treatment of gastric cancer following dital gastric Resection. In a study by Porie 50% of Gastro-Js were BII’s






