Download
1 / 1
10 likes | 172 Vues
ECCO 15 and ESMO 34 Sep 20-24, 2009. OMIT Bretagne /Pays de la Loire. Management of unresectable metastatic colorectal cancer (MCRC) in the real world with successive regimens with targeted therapies (bevacizumab and cetuximab) : the experience of the OMIT Bretagne Pays de la Loire.

E N D
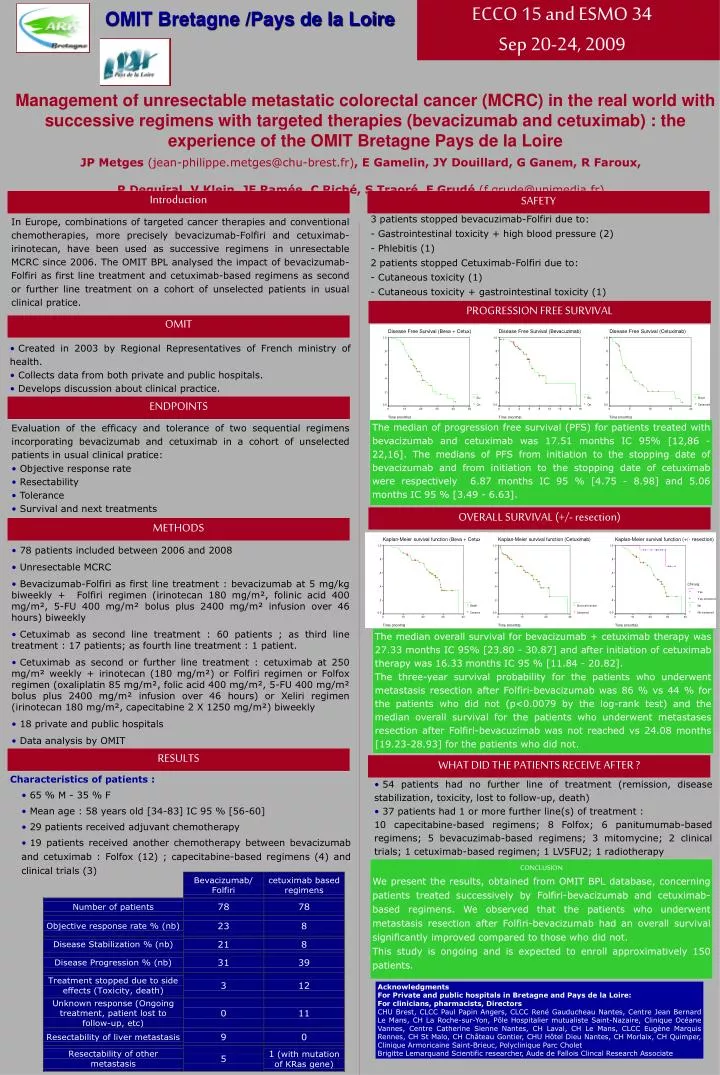
ECCO 15 and ESMO 34 Sep 20-24, 2009 OMIT Bretagne /Pays de la Loire Management of unresectable metastatic colorectal cancer (MCRC) in the real world with successive regimens with targeted therapies (bevacizumab and cetuximab) : the experience of the OMIT Bretagne Pays de la Loire JP Metges (jean-philippe.metges@chu-brest.fr), E Gamelin, JY Douillard, G Ganem, R Faroux, P Deguiral, V Klein, JF Ramée, C Riché, S Traoré, F Grudé (f.grude@unimedia.fr) Introduction SAFETY In Europe, combinations of targeted cancer therapies and conventional chemotherapies, more precisely bevacizumab-Folfiri and cetuximab-irinotecan, have been used as successive regimens in unresectable MCRC since 2006. The OMIT BPL analysed the impact of bevacizumab-Folfiri as first line treatment and cetuximab-based regimens as second or further line treatment on a cohort of unselected patients in usual clinical pratice. 3 patients stopped bevacuzimab-Folfiri due to: - Gastrointestinal toxicity + high blood pressure (2) - Phlebitis (1) 2 patients stopped Cetuximab-Folfiri due to: - Cutaneous toxicity (1) - Cutaneous toxicity + gastrointestinal toxicity (1) PROGRESSION FREE SURVIVAL OMIT • Created in 2003 by Regional Representatives of French ministry of health. • Collects data from both private and public hospitals. • Develops discussion about clinical practice. ENDPOINTS The median of progression free survival (PFS) for patients treated with bevacizumab and cetuximab was 17.51 months IC 95% [12,86 - 22,16]. The medians of PFS from initiation to the stopping date of bevacizumab and from initiation to the stopping date of cetuximab were respectively 6.87 months IC 95 % [4.75 - 8.98] and 5.06 months IC 95 % [3.49 - 6.63]. • Evaluation of the efficacy and tolerance of two sequential regimens incorporating bevacizumab and cetuximab in a cohort of unselected patients in usual clinical pratice: • Objective response rate • Resectability • Tolerance • Survival and next treatments OVERALL SURVIVAL (+/- resection) METHODS • 78 patients included between 2006 and 2008 • Unresectable MCRC • Bevacizumab-Folfiri as first line treatment : bevacizumab at 5 mg/kg biweekly + Folfiri regimen (irinotecan 180 mg/m², folinic acid 400 mg/m², 5-FU 400 mg/m² bolus plus 2400 mg/m² infusion over 46 hours) biweekly • Cetuximab as second line treatment : 60 patients ; as third line treatment : 17 patients; as fourth line treatment : 1 patient. • Cetuximab as second or further line treatment : cetuximab at 250 mg/m² weekly + irinotecan (180 mg/m²) or Folfiri regimen or Folfox regimen (oxaliplatin 85 mg/m², folic acid 400 mg/m², 5-FU 400 mg/m² bolus plus 2400 mg/m² infusion over 46 hours) or Xeliri regimen (irinotecan 180 mg/m², capecitabine 2 X 1250 mg/m²) biweekly • 18 private and public hospitals • Data analysis by OMIT The median overall survival for bevacizumab + cetuximab therapy was 27.33 months IC 95% [23.80 - 30.87] and after initiation of cetuximab therapy was 16.33 months IC 95 % [11.84 - 20.82]. The three-year survival probability for the patients who underwent metastasis resection after Folfiri-bevacizumab was 86 % vs 44 % for the patients who did not (p<0.0079 by the log-rank test) and the median overall survival for the patients who underwent metastases resection after Folfiri-bevacuzimab was not reached vs 24.08 months [19.23-28.93] for the patients who did not. RESULTS WHAT DID THE PATIENTS RECEIVE AFTER ? • Characteristics of patients : • 65 % M - 35 % F • Mean age : 58 years old [34-83] IC 95 % [56-60] • 29 patients received adjuvant chemotherapy • 19 patients received another chemotherapy between bevacizumab and cetuximab : Folfox (12) ; capecitabine-based regimens (4) and clinical trials (3) • 54 patients had no further line of treatment (remission, disease stabilization, toxicity, lost to follow-up, death) • 37 patients had 1 or more further line(s) of treatment : • 10 capecitabine-based regimens; 8 Folfox; 6 panitumumab-based regimens; 5 bevacuzimab-based regimens; 3 mitomycine; 2 clinical trials; 1 cetuximab-based regimen; 1 LV5FU2; 1 radiotherapy CONCLUSION We present the results, obtained from OMIT BPL database, concerning patients treated successively by Folfiri-bevacizumab and cetuximab-based regimens. We observed that the patients who underwent metastasis resection after Folfiri-bevacizumab had an overall survival significantly improved compared to those who did not. This study is ongoing and is expected to enroll approximatively 150 patients. Acknowledgments For Private and public hospitals in Bretagne and Pays de la Loire: For clinicians, pharmacists, Directors CHU Brest, CLCC Paul Papin Angers, CLCC René Gauducheau Nantes, Centre Jean Bernard Le Mans, CH La Roche-sur-Yon, Pôle Hospitalier mutualiste Saint-Nazaire, Clinique Océane Vannes, Centre Catherine Sienne Nantes, CH Laval, CH Le Mans, CLCC Eugène Marquis Rennes, CH St Malo, CH Château Gontier, CHU Hôtel Dieu Nantes, CH Morlaix, CH Quimper, Clinique Armoricaine Saint-Brieuc, Polyclinique Parc Cholet Brigitte Lemarquand Scientific researcher, Aude de Fallois Clincal Research Associate