Download
1 / 15
150 likes | 248 Vues
#6 Essential Emergency Airway Care- Video Laryngoscopy. Andrew Brainard, MD, MPH, FACEM, FACEM http://www.thesharpend.org/ abrainard01@gmail.com. #6 RSI and Video L aryngoscopy. Learning Objectives Prep team/plan/room/equipment Mask seal, BVM, adjuncts, suction

E N D
#6Essential Emergency Airway Care-Video Laryngoscopy Andrew Brainard, MD, MPH, FACEM, FACEM http://www.thesharpend.org/ abrainard01@gmail.com
#6 RSI and Video Laryngoscopy • Learning Objectives • Prep team/plan/room/equipment • Mask seal, BVM, adjuncts, suction • Pre and apnoeic oxygenation • Pt Positioning • Airway assessment and plan • MOANS/LEMON • Announce “pullout criteria” • Briefing for Plan A, B, C, & D • Completes FINAL airway checklist • Call and response • <1 min • Manual InLine Stabilization • Video laryngoscopy • Indications/Contraindications • Advantages/disadvantages • Proper Technique • Confirm and secure tube • Solving difficult tube passage problems • Use suction early • Back off camera • Use prebent stylet • Pre-curve bougie • External Laryngeal Manipulation • Advance ETT off stylet • Complete Airway Audit Form • R40: 25y/o M rollover RTC • GCS 10, SaO2 98%, P 140, BP 140/70. • Agitated with head injury • In C-collar • On arrival • LEMON shows: • No facial trauma, No blood in airway, normal 3-3-2, gurgling • Predicted difficult airway: in C-collar • Consultant suggests Glidescope • Patient can only be intubated using • Manual Inline Stabilization • Suction • Videolaryngoscope • Best Look Techniques • External Laryngeal Manipulation • End scenario after tube confirmation • Discuss solving difficult tube passage
Indications for Video Laryngoscopy? • Absolute Contraindication: • Inability to oxygenate patient • Cricothyrotomy • Indicated for: • Primary • Secondary • Relative Indications: • Predicted difficult airway? • Spinal precautions? • Relative Contraindications: • Fluid in the airway (like blood or vomitus) that cannot be cleared with suction • Operator inexperience • Reserving VL as onlya rescue device is dangerous • Practice before you need it as a rescue device
Video Laryngoscopy Direct Laryngoscopy
Pre-Oxygenate >3min(Attempt to get oxygen to 100% for several minutes before RSI) • Non-Hypoxic patient • Nasal Cannula • Oxygen as high as tolerated • Rebreather Mask • Oxygen as high as tolerated • Non-Hypoxic or Hypoxic/Hypoventilating Patient • Nasal Cannula • Oxygen as high as tolerated • BVM • Mask Seal/PEEP/ETCO2
Nasal Apneic Oxygenation • Apneic Period • Nasal cannula O2% to >15 lpm • Jaw thrust / NPA / laryngoscope
Positioning • Ear-to-sternal notch level • Face parallel to ceiling • RAMP • Head up • Bed height
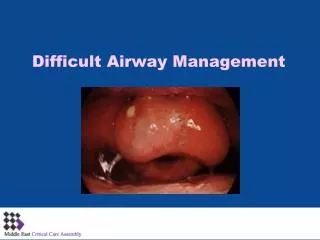
Formal Airway Assessment • LEMON • L- Look • E- Evaluate the 3-3-2 rule • 3pt fingers in the mouth • 3pt fingers under the jaw • 2pt fingers from thyroid to jaw • M- Mallampati/ Mouth • O- Obstruction • N- Neck Mobility Fluids can make video laryngoscopy more difficult
Teeth Anterior Tongue Tonsils Posterior Tongue Uvula Soft Palate Hard Palate
4 step Glidescope • Look directly at patient’s mouth • Insert midline • Use suction early • Watch mouth until tip passes out of view • Look at the screen after tip passes into posterior oropharynx. • Use screen to visualize epiglottis. • Insert tip of into vallecula • Apply upward pressure • Visualize the vocal cords and glottis • Suction if needed. • Look at the mouth • Pass the stylet’ed ETT (or a prebent bougie) into the mouth • Look again at the screen • Advance ETT off stylet into the glottis Using the Glidescope http://www.youtube.com/watch?v=7jb2tbqQ6VQ (3min)
Epiglottis-Laryngoscopy-Tube Passage #1- Prepare • Prepare Team- (EEACC #1) • Optimize pt • Oxygenate pt- (EEACC #2) • Position optimally - (EEACC #2) Prepare Glidescope • Warm up • Select blade size • ~4 for tall men • ~3 for most patients #2- Visualize Epiglottis • Mouth then Screen #3- Visualize Glottis • Place blade above vallecula • Visualize the arytenoid cartilage #4- Pass Tube • Watch mouth and insert tube • Watch screen • Re-maximize your view • Advance tube through glottic opening • Advance tube off stylet through the glottic opening More Glidescope http://www.youtube.com/watch?v=BvpUI7vOpDw (6min)
Difficulties with Glidescope? • Lubricate exterior of blade, ETT and stylet • Remember geometry • Use stylet • Prebend bougie • Don’t “Over Zoom” • Keep camera far away from glottis • Backing up camera • Keep epiglottis in view • Place the blade above vallecula • Glottis in the centre top third of screen • Manipulate patient • Elevate head, lift jaw, use ELM • Advance ETT off end of tube • Withdraw the stylet • Advance tube off end of stylet through the cords (like an IV cath) • Don’t task-fixate on the picture • Watch the sats • Prepare plan B, C, D… Common errors with glidescope: http://www.youtube.com/watch?v=0Z0s8875yc4 Difficult Video Laryngoscopy: http://prehospitalmed.com/2013/05/14/learning-from-failed-intubations-a-study-of-3-videos/ (30min)
Airway briefing and checklist Andy JoAnn Andy Chris Chris- Bimanual Fred • We have a 50y/o female victim of head trauma who needs to be intubated because she is not protecting her airway. • Based on our formal airway assessment, it is appropriate to proceed. • We will RSI with 100mg of Ketamine and 100mg of Rocuronium. • The team will be: • I’ll be team leader • JoAnn as primary airway operator • Fred will hold manual-inline c-spine stabilization • I’ll be the backup airway operator • Chris as airway assistant • Henry also push the drugs • Our plan is: • A- Video/7.5 tube w/stylet • B- Direct/bougie/7.5 tube • C- AirQsize #3.5 • D- Cric for Sats <80% and dropping • We will pullout if SaO2 drops below 93% or if we can’t see anything after 1 minute. • We will re-oxygenate after each attempt. • Everyone understand their roles? • Questions or suggestions? • Is everyone ready to complete the checklist in less than a minute? Andy 14
Brief Video Laryngoscopy References: • Glidescope, 4-step technique: https://vimeo.com/38937634 • Levitan, Four Secrets to video laryngoscopy: http://www.epmonthly.com/features/current-features/four-secrets-to-video-laryngoscopy-/ • Mihn, Learning from failed intubations- a study of 3 videos: http://prehospitalmed.com/2013/05/14/learning-from-failed-intubations-a-study-of-3-videos/ • John Doyle Eight Intubations using the Color GlideScope Video Laryngoscope http://www.youtube.com/watch?v=BvpUI7vOpDw (Accessed on 24/4/2013) • Levitan RM, Heitz JW, Sweeney M, Cooper RM. Ann Emerg Med. 2011 Mar;57(3):240-7. The complexities of tracheal intubation with direct laryngoscopy and alternative intubation devices.