Download
1 / 64
750 likes | 1.56k Vues
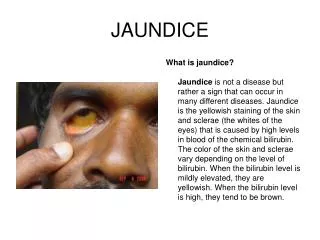
lek. Anna Skubała Department of Infectious , Tropical Diseases and Parasitoses . Infectious Diseases and Hepatology Clinic. JAUNDICE. Basic classificATION. MECHANICAL JAUNDICE. NON-OBSTRUCTIVE JAUNDICE. Bile ducts ( intra - or extrahepatic ) involved Mechanical blockage

E N D
lek. Anna Skubała Department of Infectious, TropicalDiseases and Parasitoses. InfectiousDiseases and HepatologyClinic JAUNDICE
Basic classificATION • MECHANICAL JAUNDICE • NON-OBSTRUCTIVE JAUNDICE
Bile ducts (intra- orextrahepatic) involved Mechanicalblockage Cholelithiasis(gall stones) – Cholecystolithiasis – Chledocholithiasis Pancreatolithiasis Neoplasmatic tumor aroundduodenum, caputpancreas, duodenalpapilla (Vater’spapilla) Primarycholangiocarcinoma Infectionsinthe same places MECHANICAL JAUNDICE
Infectious (HBV, HCV, HAV, otherhepatotropicviruseslike CMV, EBV) Autoimmunologic (AIH, PBC, PSC) Genetic (Wilson’sdisease, hemochromatosis, Gilbert’ssyndrome, Budd-Chiarisyndrome, Crigler-Najjarsyndrome) Toxic (paracetamol, otherdrugs and chemicals, mushrooms, alcohol) Non-obstructivejaundice
Alwaystakeintoconsideration a possibility of otherinternaldiseaseslike: • Heartinsufficieny • Hemolyticanaemia • Erytrocytes’ impairement (artificialheartvalve, hemodialysis, DIC, haemolytic-uraemicsyndrome) • Severeinfections (sepsis, malaria, toxoplasmosis) • Severeburns • Hipersplenism And oncologicdiseases: • HCC hepatocellular carcinoma • Metastases to hepar • Limphoproliferativesyndromes, lymphomas Non-obstructivejaundice
Autosomalrecessive Excessivecopperaccummulation, mainlyinliver, due to defectiveprotein, whichisresponsible for transport of Cu inthehepatocytes’ membrane Cu is not excretedwith bile Cu accumulateinliver, brain, kidneys and incornea – impairment of thoseorgans
First manifestationsinchildhoodorearlyadulthood Differentconstelation of signsindifferentpatients Hepatomegaly, hepatitis, livercirrhosiswithsigns of portal hypertension, acuteliverfailure Parkinson’ssyndrome(intention tremor, bradykinesis, stiffness, dyzarthria), epilepticseazures, migrainheadache, hypersalivation, sleeplessness, personalitydisturbances, affectivedisturbances, psychoses Kayser-Fleischer rings, cataract, Fanconisyndrome, cardiomiopathy, heartrythmdisorders, osteoporosis, arthritis, pancreatitis, retardedsexualmaturation, infertility, lack of menstruation, habitualmiscarriages, hypothyroidism, hypoparathyroidism, hemolysiswithjaundice
AST, ALT Serum ceruloplasmin Total serum copperconcentration In histologicexaminatoion – uncharacteristicchanges, Cu concentration
Kayser-Fleischer rings Decreasedceruloplasminconcentration Liverimpairmentsignsorneurologicmanifestations Criteria:
liver biopsy with assessment of copper contentin the specimen
If the diagnosis is confirmed – test 1st degree family members
alcohol abstinence NO: nuts, chocolate, mushrooms, liver, mussels continouspenicylamine treatment zinc Treatment:
In case of acute liver failure or in unstable cirrhosis resistant to treatment – liver transplantation Regular follow-up visits
autosomalrecessive mutation in the gene responsible for membrane protein impairment of hepcidine production – protein inhibiting iron absorption in GI tract and iron release from the macrophages excessive iron absorption causes its accumulation in organs like: liver, pancreas, heart, joints
clinicalmanifestations – more often in men firstsymptoms > 20 years of age in men and > 40 years of age in women early symptoms: weakness, libido decline, arthralgia (hands, wrists) later signs: the effect of chronic hepatitis or liver cirrhosis, cardiomiopathy, pancreas impairment, hormonal disorders (hypopituiarismus, hypothyroidism) progressive disease liver cirrhosis 1/3 of the patients reveal hepatocarcinoma (HCC)
Fe, ferritin AST, ALT (ALT > AST) CT, MRI – liver cirrhosis
liver biopsy– assessment of disease advance, fibrosis (prognosis); excessive iron accumulation in hepatocytes, fibrosis, cirrhosis genetic tests – mutations searched by PCR (also 1st degree family members of patients with hemochromatosis)
restrictive meat consumption alcohol abstinence avoiding dietary supplements containing iron and vit. C bloodletting deferoxamine Treatment:
Alcohol-relatedsteatosisof theliver (fattydegeneration)– asymptomatic; reversible Alcohol-relatedhepatitis – fatigue, nausea, vomiting, pain in right subcostal area, hepatomegaly, tenderness of liver (>80%), ascites (up to 80%), jaundice (> 60%), hepatic encephalopathy (45%), temperature (up to 30%) Cirrhosisof liver due to alcohol abuse Stages:
Women are more susceptible to negative effects of alcohol smaller dose faster progress
GGTP ALT, AST – sometimes (AST/ALT >= 2) ALP, Fe , bilirubin prothrombintime – elongation electrolytedisorders (hypoNa, hypoK; hypoMg) leucocytosis, macrocyticanaemia, trombocytopaenia Diagnosis:
rule out other possible causes of liver dysfunction history of alcohol abuse GGTP ultrasonographic picture of liver Criteria:
alcohol abstinence treatment of malnutrition and other defficiences connected with alcohol abuse treatment of electrolytes disorders glycocorticosteroidsif severe course of the disease with encephalopathy treatment of cirrhosis and liver failure complications Treatment:
chronic, progressive hepatitis in people who do NOT abuse alcohol histopatologicchanges similar to those in alcoholic liver disease
Causes: A. Metabolic disorders: • metaboicsyndrome • DM • obesity • protein malnutrition • excessive weigh loss (zespoleniaomijającejelitacienkiegoiżołądka, excision of a large part of intestine, long-lasting starvation, malabsorption syndrome, celiakia, unspecific enteritis, pancreas diseases) • total, long-lasting parenteral feeding • lipids metabolism disorders • chorobyspichrzeniowe (Wolmans disease, Niemann-Pick disease) • Tay-Sachs disease • Gaucherdisease • Wilson's disease • hemochromatosis • glikogenoses B. Drugs: • Amiodaron • Diltiazem • Tamoxifen • GKS • Warfarin • ARV drugs • antibiotics (tetracycline, bleomycin) • Cytostatics • large doses of vit. A • Metotrexat • salicylanes, ASA C. Hepatotoxins: • carbon tetrachloride • Phosphorus • alpha-amanitin D. Infections: • HCV • HDV E. Other: • Reye's syndrome • pregnancy complication • eclampsia
usually asymptomatic fatigue weakness discomfort in right upper abdominal quadrant hepatomegaly(<75%) or splenomegaly (<25%) other signs of portal hypertension (rarely) Symptoms:
AST, ALT (AST/ALT <1) dyslipidaemia hyperglycaemia hypoalbuminaemia prothrombintime elongation Fe, ferritin GGTP, bilirubin liver biopsy Diagnosis:
causative – e.g. metabolicsyndrome treatment of liver cirrhosis complications Treatment:
hepatic veins thrombosis could also contain VCI thrombosis impaired blood drainage from the liver
myeloproliferativeneoplsms (polycythaemia, nadpłytkowość) stanynadkrzepliwości oral contraceptives idiopathic Causes:
If comprises one of the hepatic veins and the collateralcirculation is well developed – asymptomatic If all 3 hepatic veins involved – acute liver failure, with fast growing ascites Usually sub-acute or chronic: hepatomegaly, ascites, jaundice, liver failure symptoms, peripheral oedema
dopplerultrasonography CT angio-MRI Diagnosis:
causative– ifpossible chronicanticoagulanttreatment acute: liver transplantation Treatment:
chronic necrotico-inflammatory process of liver unknownethiology increased serum gamma-globulin concentration presenceof autoantibodies
no age limit, most common in okrespokwitana and between 40. - 60. years of age 4 times more common in women
asymptomatic acute or chronic hepatitis
most common symptom – fatigue jaundice rarely acute liver failure more aggressive and treatment resistant in children and young adults co-existingotherautoimmunologicdiseases