Download
1 / 30
320 likes | 492 Vues
Interventions for preventing unintended pregnancies among adolescents. Systematic Review. NU517 Clinical Scholarship for Evidence Based Practice Cornelia C. Campbell (Roline) 22 September 2010. Clinical problem. Purpose of this systematic review. Unintended pregnancy among adolescents

E N D
Interventions for preventing unintended pregnancies among adolescents Systematic Review NU517 Clinical Scholarship for Evidence Based Practice Cornelia C. Campbell (Roline) 22 September 2010
Clinical problem Purpose of this systematic review • Unintended pregnancy among adolescents • Public health challenge • Developed & developing countries • Numerous prevention strategies have been employed • Uncertainty exists regarding the effect of these strategies • To assess the effects of primary prevention interventions on unintended pregnancy in adolescents Problem and Purpose
Search process: • Used Cochrane Fertility Regulation Group methods • Searched: • Electronic resources • Other resources Sample selection process
Cochrane Central Register of Controlled Trials (CENTRAL) • Specialist Health Promotion Register, Social Science Research Unit (SSRU) • Databases: • La Literatura Latinoamericana y del Caribe de Informacion en Ciencias de la Salud (LILACS) (Database 2008) • Social Science Citation Index (1981 – June 2007) • Science Citation Index (1981 – June 2007) • MEDLINE (1966 – Dec 2008) • EMBASE (1980 – Nov 2008) • Dissertations Abstracts Online (http://library.dialog.com/bluesheets/html/bl0035.html) • The Gray Literature Network (http://www.asti.gov/graylit/) • HealthStar • PsycINFO • CINAHL • POPLINE Sample selection process (cont.)a. Electronic resources
Contacted individual researchers • Contacted National & International research institutes, centers and organizations working in field of adolescent reproductive health • Goal to obtain info on unpublished and/or ongoing trials • Read through references of all selected studies • Ensure no relevant studies left out Sample selection process (cont.)a. Other resources
Critique selection of databases • Appropriate = yes • Focus on information resources with special interest in adolescent reproductive health • Comprehensive = yes • Looked at registers, databases, citation indexes and gray literature. • Also contacted organizations and individuals • Reviewed references • Search methods (FYI) • No language restrictions (Translations sought were needed) • No restrictions on journal of publication • No country or geographical restrictions • Search terms listed in appendix
Inclusion Exclusion • Individual and cluster randomized controlled trials (RCTs) which evaluated interventions aimed at : • Increasing knowledge and attitudes relating to risk of unintended pregnancies, • Promoting delay in the initiation of sexual intercourse and • Encouraged consistent use of birth control methods to reduce unintended pregnancies • Participants were adolescents aged 10-19 years. • Quasi experimental studies • Non-randomized controlled studies • None of the desired outcomes were measured, • Participants were pregnant • Participants were couples • Participants were above the required age range • Did not use the desired intervention • Stated method of randomization not adequate. Sample selection process (cont.)Inclusion and exclusion criteria
Clearly described in the report = yes • Six parameters used: • Generation of allocation sequence • Concealment of allocation • Blinding • Incomplete outcome data • Selective outcome reporting • Other sources of bias • Set of criteria is well defined and appears to be defensible Quality AppraisalProcess used to evaluate the methodological quality of the research reports
This criterion was defined as: • “Yes” when: • Method described was suitable to prevent bias • Examples: computer generated random numbers; table of random numbers; drawing lots • “Unclear” when: • Method was not described but trail was described as “randomized” • “No” when: • Sequences could be related to prognosis • Examples: case record number; date of birth; day, month or year of admission Methodological quality1. Generation of allocation sequence
This criterion was defined as: • “Yes” if: • Evidence that authors took proper measures to conceal allocation (example = centralized randomization) • “Unclear” if: • Authors did not report concealment scheme, or • Reported a concealment approach that is unclear • “No” if: • Concealment of allocation was inadequate Methodological quality2. Concealment of allocation
This criterion was defined as: • “Yes” if: • Evidence of no blinding and outcomes are unlikely to be influenced by lack of blinding, or • Blinding of participants and key study personnel was ensured and unlikely that it was broken, or • Outcome assessment was blinding and non-blinding of others unlikely to introduce bias • “Unclear” if: • Insufficient information, or • Outcome not addressed • “No” if: • No blinding and outcome likely to be influenced by blinding, or • Blinding carried out but likely to be broken Methodological quality3. Blinding
This criterion was defined as: • “Yes” if: • Evidence of no missing outcome data, or • Reason for missing outcome data unlikely to be related to true outcome, or • Missing outcome data balanced in numbers across intervention groups and with similar reasons across groups for dichotomous outcome data • Proportion of missing outcome data not enough to have clinically relevant impact • “Unclear” if: • Insufficient reporting of attrition/exclusions to permit judgment of “yes” or “no” • “No” if: • Reason for missing outcome data likely related to true outcome • Proportion of missing outcome data enough to induce clinically relevant bias Methodological quality4. Incomplete outcome data
This criterion was defined as: • “Yes” if: • All of the pre-specified (primary & secondary) outcomes of interest in the review have been reported as stated in protocol, or • Evident that published reports include all expected outcomes • “Unclear” if: • Insufficient information to permit judgment of “yes” or “no” • “No” if: • Not all of the study’s pre-specified outcomes have been reported, or • One/more primary outcomes were reported using measurements, analyses or subsets of data which were not pre-specified, or • One/more reported primary outcomes were not pre-specified • One/more outcomes of interest are reported incompletely • Study report fails to include results for key outcome that would be expected to have been reported Methodological quality5. Selective outcome reporting
This criterion was defined as: • “Yes” if: • Study is free of other sources of bias • “Unclear” if: • Insufficient information to assess if an important risk of bias exists, or • Insufficient rationale or evidence that an identified problem will introduce bias • “No” if: • Has extreme baseline imbalance, or • Claimed to have been fraudulent, or • Stopped early due to some data-dependent process, or • Potential source of bias related to specific study design used Methodological quality6. Other sources of bias
Data extracted from each study • Methods • Participants • Interventions • Outcome measures and results • Missing data Data Analysis
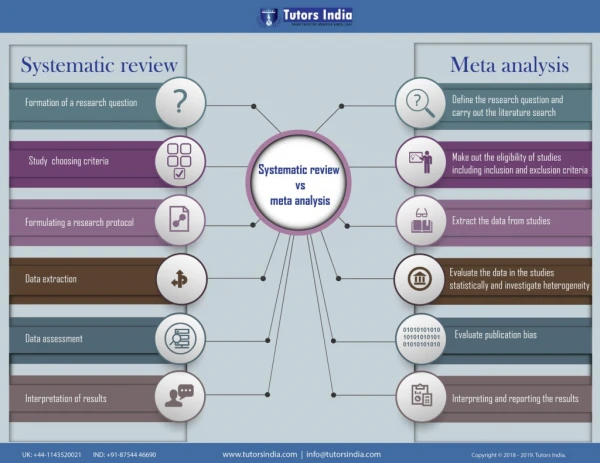
Were individual patient data or aggregate data used in the analysis? • Both • 11 studies randomized individuals • 27 studies randomized clusters (schools, classrooms, communities) • 3 studies had a mix of individual and cluster randomized data • Does it include meta-analysis or meta-synthesis? • Meta-analysis was performed using 10 of the original 41 included studies Data Analysis
Models used included: • Fixed Effect Model (FEM) and • Random Effects Model (REM) for cases where heterogeneity were detected • Assessment of effect size and confidence interval • 95% Confidence Intervals (CI) • Relative Risk (RR): • RR < 1 (negative RR) favors treatment/intervention • RR > 1 (positive RR) favors no treatment/intervention Data synthesis
Primary outcomes: • Unintended pregnancy • Secondary outcomes: • Report changes in knowledge and attitudes about the risk of unintended pregnancies • Initiation of sexual intercourse • Use of birth control methods • Abortion • Childbirth • Morbidity related to pregnancy, abortion or childbirth • Mortality related to pregnancy, abortion or childbirth • Sexually transmitted infections (including HIV) Outcome measures
2 RCT’s found the risk of UP lower in intervention group • Results approached statistical significance (p = 0.069) • RR 0.72 (95% CI 0.51 – 1.03) • 5 Cluster RCTs found risk of UP lower in intervention group • Results were not statistically significant (p = 0.083) • RR 0.50 (95% CI 0.23 – 1.09) • Sensitivity analysis excluding trials with high attrition rates found significantly lower risk of UP in intervention group • RR 0.20 (95% CI 0.10 – 0.39) • Sensitivity analysis combining cluster RCTs with individual RCTs found statistically significant lower risk of UP in intervention group. • RR 0.49 (95% CI 0.33 – 0.74) ResultsEffects of Multiple Interventions onPrimary outcome - Unintended pregnancy (UP)
Effect of contraceptive promotion • Two individually RCTs indicated no statistically significant difference between intervention and control group • RR 1.01 (95% CI 0.81 to 1.26) ResultsEffects of single Intervention onprimary outcome – unintended pregnancy
No results reported None of the included RCTs analyzed effect of multiple interventions on STDs ResultsEffects of multiple Interventions onsecondary outcome – sexually transmitted diseases
Effect of Contraceptive Use on STD’s • One individual RCT found lower rate of STD among members of intervention group • RR 0.52 (95% CI 0.20 to 1.31) • Two cluster RCTs measured reporting of STDs among intervention group members compared to control group members • RR 0.72 (95% CI 0.26 to 2.02) • Neither individual nor cluster RCTs yielded statistically significant findings • Effect of Contraceptive Promotion on STD’s • Two individual RCTs indicated no statistically significant difference found in risk of STDs between intervention group & control group • RR 0.92 (95% CI 0.75 to 1.13) ResultsEffects of Single Intervention on secondary outcome –Sexually transmitted diseases
Results were consistent across those studies that measured this outcome • Findings were not always statistically significant • Combined intervention effect was not statistically significant • Authors concluded that: • Limited information suggests use of multiple interventions can reduce rates of unintended pregnancies in adolescents Results & ConclusionsPrimary outcome: Unintended pregnancy
No conclusive determination could be madedue to: • Insufficient data • Variations in methods of reporting Results & Conclusionssecondary outcome: Sexually transmitted diseases
Implications for nursing practice • Concurrent use of multiple interventions (education, skill-building & contraception promotion) reduces risk of unintended pregnancy in adolescents • However, offers little evidence about effect of each of these interventions offered alone • Overall: evidence remains inconclusive Implications
What changes in practice were proposed? • None • Evidence cannot be used as basis to recommend the use or discontinuation of interventions Implications
How can nurses use the findings in practice? • Although findings does not change practice, nurses can use it in their role as researchers by: • Developing uniform approach in reporting outcomes • Conducting more trials in low-income countries to provide a balance of evidence with regard to obvious disparities in socio-cultural and economic situations. Implications
Oringanje, C., Meremikwu, M. M., Eko, H., Esu, E., Meremikwu, A., & Ehiri, J. E. (2009). Interventions for preventing unintended pregnancies among adolescents. Cochrane Database of Systematic Reviews, (4). doi: 10.1002/14651858.CD005215.pub2 Reference