Download
1 / 5
50 likes | 249 Vues
Radiothérapie du glioblastome : comparaison de 2 méthodes de contourage (RTOG versus MD Anderson Cancer Center) [1]. Recommandations de contourage. Groupe A RTOG. Groupe B MD Anderson Cancer Center. Phase initiale RT 40 Gy en 20 fractions Phase de boost RT 20 Gy en 10 fractions

E N D
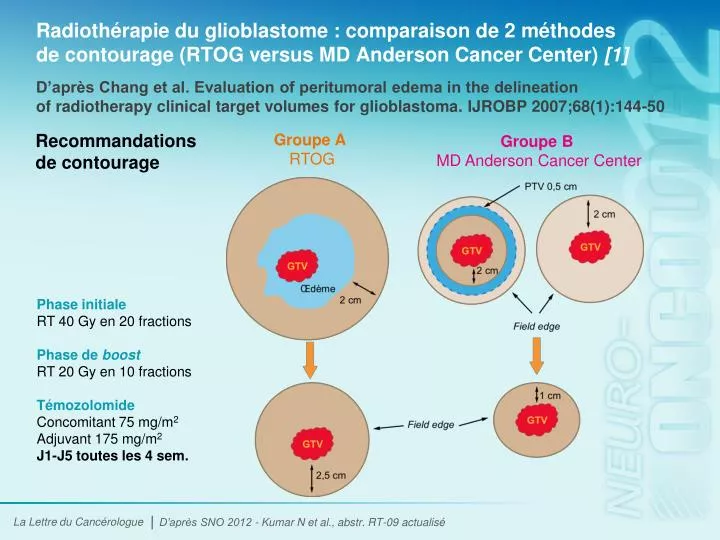
Radiothérapie du glioblastome : comparaison de 2 méthodes de contourage (RTOG versus MD Anderson Cancer Center) [1] Recommandations de contourage Groupe A RTOG Groupe B MD Anderson Cancer Center Phase initiale RT 40 Gy en 20 fractions Phase de boost RT 20 Gy en 10 fractions Témozolomide Concomitant 75 mg/m2 Adjuvant 175 mg/m2 J1-J5 toutes les 4 sem. D’après SNO 2012 - Kumar N et al., abstr. RT-09 actualisé D’après Chang et al. Evaluation of peritumoral edema in the delineation of radiotherapy clinical target volumes for glioblastoma. IJROBP 2007;68(1):144-50
Radiothérapie du glioblastome : comparaison de 2 méthodes de contourage (RTOG versus MD Anderson Cancer Center) [2] • Étude de phase II prospective et randomisée (d’avril 2010 à octobre 2011) • 50 patients inclus atteints d’un glioblastome (25 par bras) • Traitement par RT • 2 groupes, en fonction de la méthode de contourage • Groupe A : méthode du RTOG • Groupe B : méthode du MD Anderson Cancer Center • Dose totale de RT : 60 Gy (30 fractions sur 6 sem.) • Témozolomide en concomitant (75 mg/m2) et en adjuvant (175 mg/m2 à J1-J5 toutes les 4 sem.) • Critères principaux : mode de rechute et qualité de vie D’après SNO 2012 - Kumar N et al., abstr. RT-09 actualisé Méthodologie et caractéristiques initiales des patients
Radiothérapie du glioblastome : comparaison de 2 méthodes de contourage (RTOG versus MD Anderson Cancer Center) [3] • Volumes irradiés x 2 dans le groupe A • Modes de rechute (centrale, infield ou marginale) comparables dans les 2 groupes : centrale +++ • Qualité de vie meilleure dans le bras B D’après SNO 2012 - Kumar N et al., abstr. RT-09 actualisé Résultats
Radiothérapie du glioblastome : comparaison de 2 méthodes de contourage (RTOG versus MD Anderson Cancer Center) [4] • Meilleurs résultats obtenus avec la technique de contourage du volume cible des glioblastomes recommandée par le MD Anderson Cancer Center versus la technique du RTOG en termes de • Qualité de vie • SSP • SG • Modes de rechute comparables dans les 2 groupes • Limites de l’étude • Étude monocentrique • Faible effectif • Manque de données (suivi médian, statut MGMT) Conclusion D’après SNO 2012 - Kumar N et al., abstr. RT-09 actualisé
Abréviations CT : chimiothérapie EORTC :European Organisation for Research and Treatmentof Cancer HTA : hypertension artérielle ITT : intention de traiter MGMT : MethylGuanine-DNAMethylTransferase MMSA :Mini-Mental State Examination PS : Performance Status RCT : radiochimiothérapie RPA : RecursivePartitioningAnalysis RT : radiothérapie RTOG : Radiation TherapyOncology Group SG : survie globale SSP : survie sans progression VEGF :VascularEndothelialGrowth Factor