Download
1 / 43
430 likes | 436 Vues
Explore the functions, receptors, and disorders associated with neurotransmitters and peptide hormones such as dopamine, serotonin, oxytocin, and more. Learn about the progression and treatment options for Parkinson's disease and schizophrenia.

E N D
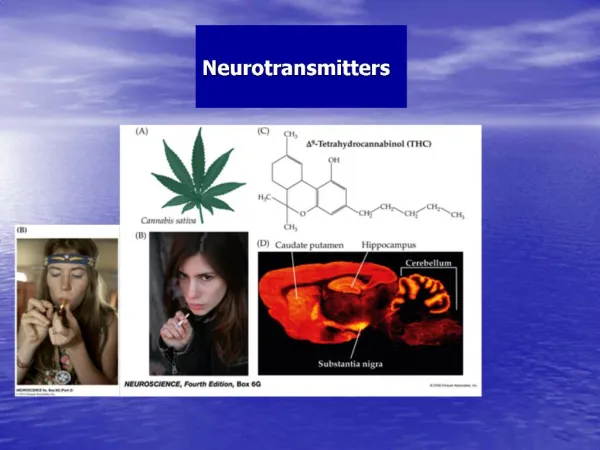
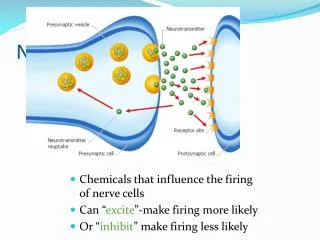
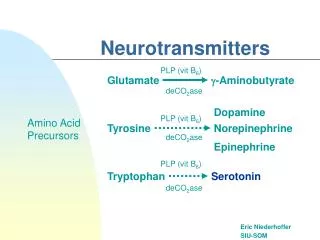
Neurotransmitters • Neuropeptides • Opioid peptides • Enkephalins (ENK) • Endorphins (END) • Peptide Hormones • Oxytocin (Oxy) • Substance P • Cholecystokinin (CCK) • Vasopressin (ADH) • Neuropeptide Y (NPY) • Brain-derived Neurotrophic factor • Hypothalamic Releasing Hormones • GnRH • TRH • CRH • Lipids • Anandamide • Gases • Nitric Oxide (NO) • Amines • Quaternary amines • Acetylcholine (ACh) • Monoamines • Catecholamines • Epinephrine (EPI) • Norepinephrine (NE) • Dopamine (DA) • Indoleamines • Serotonin (5-HT) • Melatonin • Amino acids • Gamma-aminobutyric acid (GABA) • Glutamate (GLU) • Glycine • Histamine (HIST)
Noradrenergic Receptors • Alpha 1 receptors • Smooth muscle • Skin • GI tract • Kidney • brain • Alpha 2 receptors • brain • Beta 1 receptors • Heart • kidneys • Beta 2 receptors • Lungs • GI tract • Liver • uterus • Vascular smooth muscle • Skeletal muscle • Beta 3 receptors • Fat cells All metabotropic
Beta Blockers • Cardia arrhythmias • Second Heart Attack • Hypertension
Ascending Reticular Activating System (ARAS) Arousal Center
Rats showed increased time awake after administration of small amounts of either an α1- or a β-adrenergic agonist
Dopaminergic (DA) System 1Mesolimbic * Ventral Tegmental Area (VTA)
Dopaminergic (DA) System 2Mesostriatal * Basal Ganglia
Dopaminergic Receptors • D1 receptors • D2 receptors • D3 receptors • D4 receptors • D5 receptors
Dopaminergic Synapse • Tyrosine • Tyrosine Hydroxylase • DOPA • Aromatic Amino Acid Decarboxylase • Dopamine Transporter • Vesicular Monoamine Transporter • D2 Autoreceptor
Parkinson’s Disease • A chronic, progressive, neurodegenerative disorder. • Although there are genetic and environmental risk factors, a definitive cause has not yet been discovered. • Risk of PD increases with age, but an early-onset variant occurs before age 40.
Parkinson’s Disease Tremors at Rest occurs when limbs are relaxed, and disappears with intentional movement Akinesia difficulty in initiating movement Bradykinesia slowing of movement in general Parkinson’s Disease Dimentia slow decay of brain function
Parkinson’s Disease Progression Stage 1: Degeneration starts in the dorsal motor nucleus of the vagus and the anterior olfactory structures, resulting in loss of sense of smell Stage 2: Degeneration then moves to the rapheand locus coeruleus Stage 3: Degeneration of the substantia nigra, amygdala, and nucleus basalis. Motor symptoms begin at this stage Stage 4: Degeneration of temporal lobe mesocortex. Stage 5: Degeneration of the temporal lobe, sensory association, and premotor areas. Stage 6: Degeneration of the primary sensory function and motor areas.
Selective loss of pigmented dopaminergic cells occurs in the substantia nigra
The effects of Parkinson’s disease on motor control pathways
Treatment Options Levodopa (l-DOPA), a metabolite of the amino acid tyrosine, is the immediate precursor of DA in its metabolic pathway. Side effects include motor fluctuations and dyskinesias—unwanted movements like severe tics Monoamine oxidase inhibitors (MAOIs) prevent breakdown of DA, NE, and EPI. Catechol-O-methyltransferase(COMT) inhibitors prevent breakdown of DA in the synapse but are given only as adjuncts to l-DOPA. DA receptor agonists with longer half-lives than l-DOPA, and different side effects, including impulse control disorders, such as compulsive gambling. The drug amantadine (Symmetrel) as monotherapy or to decrease dyskinesias related to l-DOPA. It is an NMDA receptor antagonist. Statin drugs for lowering cholesterol may reduce the risk of developing PD by improving heart health and increasing anti-inflammatory effects. DA receptors are up-regulated by statin therapy.
Schizophrenia Onset can be slow or sudden Typically exists chronically Affects ~1% of population Diagnosis must have at least two symptoms for more that 1 month
Schizophrenia Symptoms • Positive Symptoms (abnormal states) • hallucinations (auditory, visual) • delusions (grandeur, persecution) • Negative Symptoms (insufficient functioning) • avolition (inability to initiate/persist in activities) • alogia (absence of speech) • anhedonia (inability to experience pleasure) • affectiveflattening (flat emotional response) • Disorganized Symptoms • inappropriateaffect (laughing/crying at the wrong times) • disorganizedspeech (illogical, rambling, tangential) • disorganizedbehavior (catatonia, agitation/immobility)
Schizophrenia Subtypes • Paranoid Type • hallucinations • delusions • Catatonic Type • unusual motor responses • remaining in a fixed position • excessive activity or rigidity • echoing words or movements of others • Disorganized Type • speech problems • behavior problems • flat or inappropriate affect
Schizophreni Genetic Risk by Relatedness • The Evidence: • Family History • Twin Studies • monozygotic (50%) • same handed (92%) • dizygotic (15%) • both are carriers • Adopted Children • more like bioparents • Single Gene? • Probably not
Brain Structure AbnormalitiesReduced Hippocampus and Amygdala Affected Normal Affected Normal
Cortical gray matter loss During adolescence, a period of significant brain development, excessive synaptic pruning can result in loss of cortical gray matter.
Brain Structure AbnormalitiesHippocampal Pyramidal Cell Disorganization Reelinis a glycoprotein secreted by neurons, that guides neuron positioning during fetal brain development.
Brain Structure AbnormalitiesAtypical Frontal Lobe Functioning • Evidence: • smaller forebrain • smaller cerebral cortex • smaller dorsolateral prefrontal cortex • fewer cortical neurons • smaller cortical neurons • abnormal neuronal development • neurons remain in white matter • fail to arrange in neat order • abnormal CAMs • less metabolic activity • hypofrontality • failure to increase activity following task • abnormal EEGs
Relevant Neural Pathways • Mesolimbic pathway • affects positive symptoms. • Mesocortical pathway • cognitive and negative symptoms. • Nigrostriatal pathway • motor side effects. • Tuberohypophyseal pathway • regulates pituitary hormone secretion; neuroendocrine effects.
Neurobehavioral Hypothesis • Maternal/Fetal Evidence: • extensive maternal bleeding • prolonged labor • delivery complications • low birth weight • low head circumference • body length:body weight • multiparity • Anectodal Evidence • Dutch births during WWII • Season of birth effect • higher for winter pregnancies • parallel with virus exposure
Dopamine Hypothesis of Schizophrenia Abnormal levels of Dopamine lead to the schizophrenic symptoms • 1. Amphetamine Psychosis • Chronic users develop schizophrenic symptoms • paranoia, delusions of persecution, auditory hallucinations • Amphetamine exacerbates schizophrenic symptoms • Amphetamines promote the release of catelcholamines • particularly dopamine • 2. Antipsychotic Drugs • chlorapromazine is a dopamine antagonist and antipsychotic • block specifically D2 and D4 receptors in the limbic system • effectiveness is related to magnitude of blockade • 3. Parkinson’s Disease • some patients receiving L-dopa become psychotic • some schizophrenic patients on antipsychotics develop Parkinson’s symptoms
Hypoglutamate Hypothesis • Inadequate glutamate may explain the apparent increase in mesolimbic DA and decrease in PFC. • Descending glutamatergic neurons influence both DA pathways.
Treatment options Neurolepticis an older term for antipsychotic drugs. There are many of these drugs, and none are consistently more effective than the others. An individual may respond better to one drug than to another; several may have to be tested to find the one that is most effective. The classic antipsychotic drugs are phenothiazines and butyrophenones Negative and Cognitive symptoms are more resistant to treatment. Antipsychotic drugs block D2 receptors. A strong correlation exists between ability of a drug to displace a radio-labeled ligand on DA receptors and average clinical daily dose required. The drugs also bind to other receptors, but there is no clear relationship between clinical effectiveness and binding to serotonin, α-adrenergic, histamine, or D1 receptors.
Correlation between antipsychotic drug binding to neurotransmitter receptors and clinical effectiveness • Chlorpromazine (Thorazine) first drug to find positive effects • Strong Correlation with DA 2 receptor blockers