Download
1 / 63
680 likes | 1.11k Vues
Renal Physiology, Electrolytes and Renal Failure. Daniel Shoskes MD, FRCS(C) Professor of Surgery/Urology Glickman Urological and Kidney Institute Cleveland Clinic. What you need to know:. • Electrolyte disorders • Acid-Base disorders • Water disorders • Conduit/pouch effects

E N D
Renal Physiology, Electrolytes and Renal Failure Daniel Shoskes MD, FRCS(C) Professor of Surgery/Urology Glickman Urological and Kidney Institute Cleveland Clinic
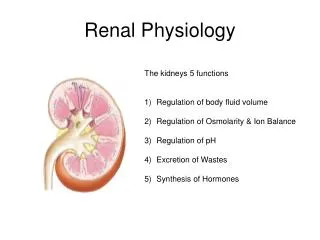
What you need to know: • Electrolyte disorders • Acid-Base disorders • Water disorders • Conduit/pouch effects • Obstruction effects • Stones/RTA • Diuretic effects • Renal anatomy • Control of vascular tone • Tubular function • Handling Na+/water • Handling K, Cl • Handling acid • Pathophysiology of renal failure
Renal Hemodynamic Definitions • Renal Blood Flow (RBF) • blood to kidneys per minute (1200 ml/min) • Renal Plasma Flow (RPF) • plasma flow to kidneys per minute (670 ml/min) • Glomerular Filtration Rate (GFR) • volume of plasma filtered per minute by the glomeruli (125 ml/min males, 100 ml/min females) • Filtration Fraction (FF) • GFR:RPF (about .18-.22)
GFR • balance of hydrostatic and oncotic pressures • hydrostatic pressure controlled by relative tonicity of pre- and post-glomerular arterioles • hyper-renin state will maintain GFR by post-glomerular arteriolar constriction • GFR may be approximated by creatinine clearance, since Cr filtered, not resorbed and minimally secreted
Equations we Hate (1) Creatinine Clearance (ml/min) = (140-age) x lean body weight (kg) ------------------------------------------- 72 x plasma creatinine (In women, above x 0.85) A. urine Cr x urine vol = ---------------------------- serum creatinine B. (total creatinine should be 1 mg/kg/hr or else inadequate collection)
GFR and Plasma Creatinine 100 • RULE OF THUMB • everytime PCr doubles, GFR drops by 50% 50 GFR (ml/min) 25 12 6 0.5 1.0 2.0 4.0 8.0 plasma creatinine (mg/dl)
MDRD Formula Glomerular Filtration Rate (ml/min/1.73m2) = 186 x (PCr) -1.154 x (age) -0.203 x (0.742 if female) x (1.210 if African American) More accurate than Cockcroft Gault in pts with renal impairment. Obviously can't ask you to calculate in exam, but know the variables
Tubular Function • maintain appropriate water, acid and electrolyte balance using passive and active mechanisms • reabsorb selectively up to 99% of the glomerular filtrate • respond to endocrine signals to make necessary changes
Proximal Tubule • resorbs 100% of glucose and amino acids, 90% of bicarbonate and 80-90% of inorganic phosphate and water • solutes active, water passive • Na reabsorption through Na-H and Na-solute active transporters • HCO3 generated in cell and absorbed with Na • ammonium secretion
Loop of Henle • early water and urea permeability, filtrate becomes hypertonic • later Na-Cl permeability • final, Na-Cl actively transported, filtrate hypotonic • creates high interstitial osmolality which permits urinary concentration
Thick Ascending Limb • the "diluting" segment • active transport of NH3 and Na • aldosterone and ADH augment Na reabsorption
Collecting Duct • provides final touches to Na, HCO3 and K • Na absorbed, K secreted (stimulated by aldosterone) • H secreted based on blood pH • NH3 secreted into lumen and can trap H to make NH4 • If ADH present, permeable to water and water is drawn by hypertonic medulla
Thiazide Diuretics • HCTZ, chlorthalidone, metolazone • inhibit Na and Cl reabsorption in distal convoluted tubule • reduce GFR and Renal Blood Flow • decrease urinary calcium
Loop Diuretics • furosemide, ethacrinic acid, bumetanide • inhibit Na/K/Cl cotransporter • increased diuresis and excretion of Na, K, Cl, Ca and Mg • reduce medullary solute content and impair urinary concentrating and diluting capacity
Disorders of Water/Sodium • Primary goals: • maintain blood pressure • excrete wastes • Mechanisms • thirst • ADH • aldosterone
Equations we Hate (2) Osmolality: Posm = 2 x plasma [Na] + [glucose]/18 + [BUN]/2.8
Equations we Hate (3) Sodium Deficit Na deficit = voldist x body weight (kg) x (125 - plasma [Na]) voldist: men = 0.5 women = 0.6
Secretion of Acid • Active Na-H pump • Glomerular filtration of buffers • HCO3, HPO4 • Ammonia (NH3) secreted in tubule combines to form non-diffusible NH4 (ammonium ion)
Acid-Base Disorders • normal arterial blood pH ranges from 7.37 to 7.43, maintained by lungs (PCO2) and kidneys (HCO3) • sudden changes tempered by buffers in blood • first determine primary disorder, then check compensation • if compensation not appropriate, suspect mixed disorder • check anion gap in metabolic acidosis (Na-(Cl+HCO3)) looking for "extra" anions (normal is 10-12)
Simple Acid-Base Disorders Metabolic Acidosis Expected pCO2 = 1.5 x [HCO3-] + 8 ± 2 Alkalosis Expected pCO2 = 6 mmHg per 10 mEq/L in HCO3 Respiratory Acidosis Acute Expected HCO3 =1 mEq/L for each 10 mm pCO2 Chronic Expected HCO3 =3.5mEq/L for each 10 mmHg pCO2 Alkalosis Acute Expected HCO3 =2 mEq/L for each 10 mm Hg pCO2 Chronic Expected HCO3- =5 mEq/L for each 10 mmHg pCO2 BUT: Nowadays most people use nomograms
Primary Disorder • pH=7.18, pCO2=14, HCO3=14, Na=140, Cl=104 • pH is low therefore acidemia • bicarb is low therefore metabolic acidosis • pCO2 is low, expected compensation • predicted pCO2 compensation 1.5*4+8=14 • anion gap 140-(104+14) = 22 (elevated) • Therefore anion gap metabolic acidosis with appropriate compensation
Respiratory Acidosis insufficient respiration consider central, mechanical and obstructive causes headache and drowsiness lead to coma and death Respiratory Alkalosis hyperventilation anxiety, fever, pain, septicemia, iatrogenic (ventilator settings) may have tetany, parasthesia Respiratory Disorders
Renal Tubular Acidosis • syndromes of metabolic acidosis from defects in tubular H secretion and urinary acidification • Type 1 (Distal, includes old 3,collecting duct) • hypo K, hypo Cl, non-anion gap met acidosis • urinary pH > 6.0 (inappropriate) • 75% of these patients get stones • Type 2 (Proximal) • same features but can acidify urine • HCO3 wasting from inability to absorb • Type 4 (Generalized Distal) • hyper K, hyper Cl • aldosterone deficiency or resistance
RTA Type 1 • Most common form • Stones usually Ca phosphate • high urine pH, Ca and low urine citrate • Diagnose by urine pH>5.5, if no met acidosis, provoke with ammonium chloride test • Treat by oral alkalinization and citrate, monitor for low K during therapy
Other RTA Forms • Type 2 • more common in children • normal citrate, no stones • growth retardation, met bone disease • treat with NaHCO3 • Type 4 • often have azotemia and hypertension • treatment aimed to reduce K
Disorders of Potassium • Mostly intracellular • Serum levels do not reflect total body content in disease states • K driven into cells by insulin, bicarb, beta-agonists • Changes in dietary intake handled by intracellular stores and urinary excretion • Excretion promoted by aldosterone, high distal Na load, chronic acidosis
Hypokalemia • Usually increased loss (GI, urine) or intracellular shift (aLKylosis = Low K) • Iatrogenic common • diuretics, laxatives, amphotericin, theophylline • hyperaldosterone states, Cushing syndrome • tachycardia, heart block, ST depression • treat underlying cause, replace K (40 mEq/hr max IV)
Hyperkalemia • usually reflects decreased renal excretion or shift out of cells (acidosis) • GI bleed, hemolysis will often exacerbate • RTA type 4, K sparing diuretics, ACE inhibitors, beta blockers • usually asymptomatic until cardiac changes • short QT, peaked T waves, ventricular arryth • mild increase, reverse predisposing cause • moderate, use binding agents (Kayexalate) • severe, give Ca/insulin/glucose drip; dialysis