Download
1 / 63
630 likes | 1.01k Vues
Evaluation, Management, and Treatment of Adverse Events of Smallpox Vaccine . Department of Health and Human Services Centers for Disease Control and Prevention December 2002. Evaluation, Management, and Treatment of Adverse Events of Smallpox Vaccine . Learning Objectives:

E N D
Evaluation, Management, and Treatment of Adverse Events of Smallpox Vaccine Department of Health and Human Services Centers for Disease Control and Prevention December 2002
Evaluation, Management, and Treatment of Adverse Events of Smallpox Vaccine • Learning Objectives: • Describe the common and serious adverse events expected after smallpox vaccination • Describe the treatment options available to clinicians when treating a patient with an adverse event to smallpox
Dryvax Smallpox Vaccine • Prepared from calf lymph containing live vaccinia virus • Contains polymyxin B, streptomycin, tetracycline and neomycin • Diluent is 50 percent glycerin and phenol as a preservative
New Smallpox Vaccines • Live vaccinia virus produced using cell culture technology • Distributed as a freeze dried powder • Do not contain antibiotics • Diluent contains glycerin and phenol
Clinical Response to Vaccination* Symptom/sign Papule Pustule Maximum erythema Scab Scab separation Time after Vacc 2-5 days 7-10 days 8-10 days 14 days 21 days *typical response in a nonimmune person
Progression of smallpox vaccination site in a non-immune person
Smallpox Vaccine Local Reactions Among Susceptible Adults Local sign • Pustule • Erythema • Induration Mean Diameter 12 mm 16-24 mm 11-16 mm
Smallpox Vaccine Local Reactions Among Susceptible Adults • Pain, swelling, erythema at vaccination site • Regional lymphadenopathy • Begins 3-10 days after vaccination • Can persist for 2-4 weeks after vaccination site heals
Smallpox Vaccine Reactions Among Susceptible Adults • Elevated temperature • 17% >100o F • 1.4% >102o F • Systemic symptoms (malaise, myalgias) • 36% sufficiently ill to miss work, school, or recreational activities or had trouble sleeping
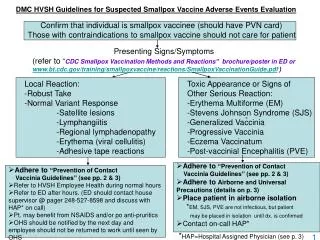
Normal Variants of Vaccine Reaction • Local edema at vaccination site • Lymphangitis • Regional lymphadenopathy (nonfluctuant) • Satellite lesions
Local Reactions Following Smallpox Vaccine • Allergic reactions to bandage and tape adhesives • Large primary vaccination reactions (“robust primary takes” – RPT) • Secondary bacterial infection
Local Reactions to Adhesive • Erythema corresponds to placement of adhesive tape • No systemic symptoms • Treat with antihistamines, NSAIDs, frequent bandage/tape change • Steroid treatment not recommended
Robust Primary Takes (RPT) • Expected variant of normal reaction • >3 inches of erythema with induration, pain, warmth • Occur in 5%-15% of recipients • Peak at day 8-10 post-vaccination • May resemble bacterial infection
Robust Primary Takes (RPT) • Observe carefully • Supportive therapy • Rest affected limb • Analgesia (non-aspirin) • NSAIDs • Usually improve in 24-48 h
Secondary Bacterial Infection • More common among children than adults • Usually Staphylococcus aureus or Group A beta hemolytic Streptococci • Anaerobic and mixed infections may occur • Evaluate with gram stain and culture • Antibiotic therapy based on culture
Major Complications of Smallpox Vaccination • Definitive studies of complications of smallpox vaccination by Lane et al, published in 1969-1970 • Led to the recommendation to cease routine smallpox vaccination in the United States
Smallpox Vaccine Adverse Reactions • Inadvertent inoculation • Eczema vaccinatum • Generalized vaccinia • Progressive vaccinia (vaccinia necrosum) • Post-vaccinial encephalitis • Other dermatologic conditions
Smallpox Vaccine Adverse Reaction Rates* *Rates per million primary vaccinations
Smallpox Vaccine Adverse Reactions • Adverse reaction rates may be higher today than in 1960s • More persons at risk because of higher prevalence of immunosuppression and eczema/atopic dermatitis • Adverse reaction rates lower among previously vaccinated persons
Rashes Following Smallpox Vaccine • Flat, erythematous, macular, or urticarial lesions • Usually do not become vesicular • Do not appear to involve viral multiplication or systemic dissemination • Occur approximately 10 days after vaccination • Resolve spontaneously within 2 to 4 days
Erythema Multiforme • May present as macules, papules, urticaria, or bulls-eye lesions • Usually appear within 10 days after vaccination • Do not progress • Do not contain vaccinia virus • Occasional Stevens-Johnson syndrome • VIG not indicated
Inadvertent Inoculation • Transfer of vaccinia virus from vaccination site to another site on the body, or to a close contact • Most frequent complication of smallpox vaccination • Occurred 25-529 cases per million primary vaccinations • Most common sites are face, eyelid, nose, mouth, genitalia, rectum • Lesions contain vaccinia virus
Inadvertent Inoculation • Uncomplicated lesions require no therapy, self-limited, resolve in ~3 weeks • VIG may speed recovery if extensive or painful genital involvement • Hand washing after contact with vaccination site or contaminated material most effective prevention
Ocular Vaccinia • May present as blepharitis, conjunctivitis, keratitis, iritis, or combination • Should be managed in consultation with an ophthalmologist • Treatment may include topical ophthalmic antiviral agents and VIG
Generalized Vaccinia • Vesicles or pustules appearing on normal skin distant from the vaccination site • Often accompanied by fever, headache, and myalgias • Occurred 23-242 cases per million primary vaccinations • Usually occur 6-9 days after vaccination
Generalized Vaccinia • Differential diagnosis • Erythema multiforme • Eczema vaccinatum • Inadvertent inoculation at multiple sites • Early progressive vaccinia • Disseminated herpes • Severe varicella
Generalized Vaccinia • Generally self-limited • Most cases do not require therapy • VIG may be considered for recurrent disease or severe disease • Lesions contain vaccinia
Eczema Vaccinatum • Generalized spread of vaccinia on the skin of a person with eczema or true atopic dermatitis, or a history of eczema or atopic dermatitis • Severity independent of the activity of the underlying eczema • Severe cases among contacts of recently vaccinated person • Occurred 10 to 39 cases per million primary vaccinations
Eczema Vaccinatum • Skin lesions may be papular, vesicular, or pustular • May occur anywhere on the body • Predilection for areas of previous atopic dermatitis • Patients often severely ill
Eczema Vaccinatum • Management • Hemodynamic support • Meticulous skin care • Early treatment with VIG • Treatment of secondary bacterial or fungal infections as needed • Lesions contain vaccinia virus
Progressive Vaccinia • Occurs almost exclusively among persons with cellular immunodeficiency • Can occur in persons with humoral immunodeficiency • Can occur following revaccination of people who have become immunosuppressed since their primary vaccination • Occurred 0.9-1.5 cases per million primary vaccinations
Progressive Vaccinia • Primary vaccination lesion does not heal • Progresses to ulcerative lesion, often with central necrosis • Little or no inflammation at the site and generally little pain • Virus continues to spread locally and through viremia • Protective T-cell count unknown
Progressive Vaccinia • Requires aggressive therapy with VIG • Antiviral therapy? • Surgical debridement? • Lesions contain vaccinia virus
Post-vaccinial Encephalitis • Usually affects primary vaccinees <12 months of age and adolescents and adults receiving a primary vaccination • Presents with any of a variety of CNS signs (e.g., ataxia, confusion, paralysis, seizures, or coma) • 15%-25% die, 25% develop neurological sequelae • Occurred 3-12 cases per million primary vaccinations
Post-vaccinial Encephalitis • Diagnosis of exclusion • Other infectious or toxic causes of encephalitis should be ruled out • Pathophysiology not well understood • CSF may have increased opening pressure, lymphocytosis, elevated protein
Post-vaccinial Encephalitis • Treatment is supportive • VIG not effective • Anticonvulsive therapy and intensive care may be required
Fetal Vaccinia • Rare complication (<50 cases reported) • Usually following primary vaccination of the mother in the second or third trimester • Fetal infection following vaccination in the first trimester would presumably result in spontaneous abortion • No known pattern of congenital malformations
Fetal Vaccinia • Death usually occurs before birth or in preinatal period • VIG may be considered if infant born alive with lesions • No known reliable intrauterine diagnostic test