Download

1 / 39
410 likes | 1.04k Vues
DISEASES OF SMALL AND LARGE INTESTINE. Diseases of small and large intestine. Disease of bowel caused by: Developmental anomalies ( Hirschsprung Disease) Vascular Disorders Diarrheal diseases Idiopathic inflammatory bowel disease Tumors Others. Developmental anomalies.

E N D
Diseases of small and large intestine • Disease of bowel caused by: • Developmental anomalies (Hirschsprung Disease) • Vascular Disorders • Diarrheal diseases • Idiopathic inflammatory bowel disease • Tumors • Others.
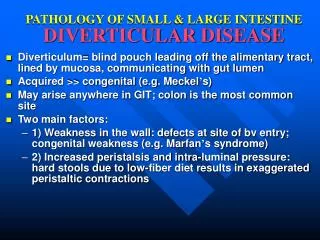
Developmental anomalies Meckel diverticulum • is the most common and innocuous of the anomalies. It results from failure of involution of the omphalomesenteric duct, leaving a persistent blind-ended tubular protrusion as long as 5 to 6 cm • in the ileum, about 80cm proximal to the ileocecal valve • Peptic ulceration in the adjacent intestinal mucosa
Developmental anomalies (Hirschsprung Disease) • during development, the migration of neural crest-derived cells along the alimentary tract arrests at some point before reaching the anus. • an aganglionic segment is formed that lacks both the Meissner submucosal and Auerbach myenteric plexuses. • This causes functional obstruction and progressive distention of the colon proximal to the affected segment. • Ganglia are absent from the muscle wall and submucosa of the constricted segment but may be present in the dilated portion.
Diarrheal diseases • Diarrheal diseases including • Acute inflammation caused by infectious organism • Malabsorption disorder. • Idiopathic inflammatory bowel disease. • Symptoms: diarrhea, dysentery and pain.
Diarrheal diseases • Diarrhea consists of daily stool production in excess of 250 g, containing 70% to 90% water. • Often accompanied by pain, discomfort, urgency and incontinence. • Dysentery is low volume painful, bloody diarrhea
Principal mechanisms of diarrhea • Secretory: • isotonic to plasma, occur in infectious conditions, neoplastic conditions and in excessive laxatives used • Osmotic: • excessive osmotic forces as Lactulose therapy and antiacids • Exudative: • output of purulent, bloody stool, occur in infectious conditions and Idiopathic inflammatory bowel disease • Malabsorption: • voluminous stool, occur in defective absorption and intraluminal digestion or lymphatic obstruction • Deranged motility
Infectious Enterocolitis • A global problem, 2.9 million death per year • Account for 1/2 of death in children younger than 5 years in some countries • In USA, about 500 infants and young children die each year because of diarrheal disease • Most common problem in traveler
Infectious Enterocolitis • Direct invasion of microbe with ulceration. • Production of enterotoxin. • Ability to adhere to mucosal lining. • Major causative agents: bacteria (E.coli), virus (calcivirus, rotavirus and Norwalk virus), fungus and protozoa.
Infectious EnterocolitisViral gastroenterocolitis • Viral infection destroy superficial epithelium in small intestine & their absorptive function • Repair by immature enterocytes with secretory function • Rotavirus: 130 million cases per year and 0.9 million deaths worldwide per year, mainly children (6-24 month)
Viral gastroenterocolitis • Rotavirus is the most common agent (140 million cases and 1 million death 1 year). • Affect children 6-24 months. • Incubation period is 2 days followed by vomiting and watery diarrhea. • Affect epithelium of the small intestine leading to secretion of water and electrolytes • May produce a flat mucosa in small intestine. • Rotavirus have intrinsic viral factor, nonstuctural protein 4 (NSP4) that induce direct diarrhea
Viral gastroenterocolitis • Caliciviruses most common virus of nonbacterial foodborne epidemic in older children and adult. • Adenovirus and astrovirus
Infectious Enterocolitis Bacterial enterocolitis • Caused by a variety of bacterial species e.g. E.coli, salmonella, shigella, campylobacter, vibrio cholerae and others. • Pathogenic mechanism: 1. Ingestion of preformed toxin e.g. C. botulism and S. aureus. 2. Infection by toxigenic organisms, e.g. E. coli, V. cholerae. 3. Infection by enteroinvasive organism e.g. salmonella, shigella or E. coli.
Infectious EnterocolitisBacterial enterocolitis • In enteroinvasive organism and toxigenic organisms bacterial replication occur • This depend on: • The ability to adhere to mucosa ( adhesins ) • The ability to elaborate toxins • The capacity to invade
Bacterial Enterocolitis Morphology • Pathologic manifestations are variable – normal (v. cholerae) to non specific inflammation and severe ulceration • E.coli - different subtypes • Entertoxigenic • The Shiga toxin - producing strain • Enteropathogenic strains • Enteroinvasive strains • Enteroaggregating strains • Shigella – distal colon, acute mucosal inflammation and erosion. • C. Jejuni– small and large intestine; villus blunting, ulceration.
Bacterial Enterocolitis • Y enterocolitis– ileum, appendix and colon; hemorrhage. and necrosis, invade Peyer patches and lymph node leading to necrotizing granulomas • Salmonella – ileum and colon; invade Peyer patches and produce linear ulceration, serosa may be normal or covered by serous, fibrinous or hemorrhagic exudate, regional lymph node may be enlarged, systemic infection (Typhoid fever) • Mycobacterium tuberculosis
Antibiotic Associated Colitis (Pseudomembranous colitis) • Acute colitis with formation of adherent inflammtory exudate. • Caused by C. difficile (produce two protein exotoxins A & B). • Occur after a coarse of broad spectrum antibiotic. • Can occur after severe necrotizing enterocolitis or in ischemic colitis.
Bacterial EnterocolitisClinical manifestation • Ingestion of preformed toxin: diarrhea, acute abdominal pain. • Infection with enteric pathogens: - Secretory enterotoxin: diarrhea - Cytotoxin or enteroinvasive process: dysentery. • Insidious infection: Yersenia and TB – subacute diarrheal illness.
Protozoal Infection Amebiasis • Entamoeba histiolytica is a common pathogen of colon. • Ingestion of cysts in the contaminated food and water. • Cysts release active amebas (trophozoites), invade large bowel mucosa and enter the submucosa (site of maximum involvement), enzymatic necrosis (flask-shaped ulcer).
Amebiasis • Gross: multiple ulcers separated by healthy-appearing mucosa, undermined by submucosal abscesses. • Micro: mucosal ulcers covered by a necrotic base. Amebas are found in the wall of the ulcer. • Complication: perforation, haemorrhage, toxic megacolon, amebic abscess.
Malabsorption Syndrome • There is increased fecal excretion of fat (steatorrhea) and the systemic effects of deficiency of vitamins, minerals, protein and carbohydrates. • Steatorrhea is passage of soft, yellowish, greasy stools containing an increased amount of fat. • Fat excretion exceeding 6 g/d is demonstrated in a 72-hour stool sample. • Disturbance of normal digestive function.
Mechanism of Malabsorption • It result from disturbance of one of these normal digestive functions • Intraluminal digestion • Terminal digestion • Transepithelial transport
Disease Causing Malabsorption • Defective intraluminal digestion e.g. pancreatic insufficiency. • Mucosal cell abnormality e.g. lactose intolerance, abetalipoproteinemia. • Reduced intestinal surface e.g. celiac disease and Crohn’s disease. • Lymphatic obstruction e.g. lymphoma. • Infection – e.g. tropical sprue. • Iatrogenic – e.g. gastrectomy.
Diseases Causing Malabsorption Celiac disease • Synonyms: nontropical sprue; gluten-induced enteropathy, gluten-sensitive enteropathy • Is a chronic disease • characteristic mucosal lesion of the small intestine with impaired nutrient absorption, which improves on withdrawal of wheat gliadins. • Occurs largely in whites (1:300 in Europe).
Malabsorption SyndromeCeliac disease • Most likely an immune reaction to gliadin • Usually diagnosed in childhood – mid adult. • Genetic background: 95% of patient have HLA-DQ2- and the remainder have HLA-DQ8-positive antigen presenting cells in the lamina properia of small intestine to CD4+ t cells • CD 8+T cells the NK cell-associated NKG2D receptor, which recognizes stress-induced molecules on epithelial cells • virus (type 12 adenovirus) • Patients have raised antibodies to gluten and IgA antiendomysial autoantibodies
Cl Normal Celiac disease
Malabsorption SyndromeCeliac Disease • Morphology • Mucosa is flattened with marked villous atrophy. • Crypts are elongated and hyperplastic. • Lamina propria: increase in chronic inflammatory cells.
Malabsorption SyndromeCeliac Disease • Immunoperoxidase shows immunocytes with IgA antigliadin antibodies. • Changes are more marked in the proximal than in the distal small intestine. • There is a 10 to 15% risk of developing GI lymphoma.
Malabsorption Syndrome Celiac Disease Clinical features Infants : Failure to thrive, diarrhea. Adults : Diarrhea, flatulence, weight loss and fatigue.
Malabsorption Syndrome Celiac Disease Diagnosis • Clinical documentations of malabsorption. • Small intestine biopsy demonstrate intestinal lesion. • Improvement of symptom and mucosal histology on gluten withdrawal from diet. • Challenge test.
Malabsorption Syndrome Tropical Sprue (post-infectious sprue) • Occurs in people living in or visiting tropical or semitropical locales. • Of unknown etiology, perhaps enterotoxigenic E.coli or haemophilus. • Most patients improve or are cured with long-term broad spectrum antibiotic therapy.
Malabsorption Syndrome Tropical Sprue (post-infectious sprue) Morphology • Variable ranging from normal to those of celiac disease. • Unlike celiac disease, injury of small intestine occur at all levels. • Deficiency of folic acid and vit. B12 – megaloblastic changes.
MalabsorptionSyndromeClinical features Malabosortion affect many organs • Hematopiotic system, anemia and bleeding • Musculoskeletal system, osteopenia and tetany • Endocrine system, amenorrhea, infertility, hyperparathyridism • Skin, purpura dermatitis hyperkeratosis • Nervous system system, neuropathy