Download

1 / 30
390 likes | 884 Vues
Splinting Seminar. Prepared by Braden Gammon R5 Department of Orthopaedic Surgery Queen’s University. Approach to Traumatic Disorders of the Extremities. ATLS – ABCDE, secondary survey If stable ->History Events surrounding/mechanism of injury (energy, positioning of limb)

E N D
Splinting Seminar Prepared by Braden Gammon R5 Department of Orthopaedic Surgery Queen’s University
Approach to Traumatic Disorders of the Extremities • ATLS – ABCDE, secondary survey • If stable ->History • Events surrounding/mechanism of injury (energy, positioning of limb) • Pain (and ability to WB), distal neurovascular symptoms (numbness/tingling) • Associated injuries incl. head injury (LOC/amnesia/seizure/nausea and vomiting) • Locking/catching, giving way/instability (esp. chronic injuries) • Pain/Disability/Function pre-injury • Hand dominance
Approach Cont. • Physical: • Look – SEADS = Swelling, Erythema, Atrophy (chronic disorders), Deformity, Skin changes (open wounds) • Feel – tenderness (bony vs. soft tissue), deformity, tests for joint effusion: ballottement, fluid bulge • Move – passive and active ROM • Special Tests: ligamentous testing, instability testing • Distal Neurovascular Status Upper Extremity: Radial (w/Posterior Interosseous N.), Median (w/Anterior Interosseous N.), Ulnar, Musculocutaneous and Axillary Nerve motor/sensory function; radial and ulnar pulses/cap refill Lower Extremity: Deep and Superficial Peroneal, Sural, Saphenous, tibial nerve motor/sensory function; posterior tibial and dorsalis pedis pulses/cap refill
Primary Management of Fractures/Dislocations • Reduce under conscious sedation or hematoma block • Basic manoeuvre is longitudinal traction and reversal of mechanism • Apply Sterile Dressing (jelonet or saline soaked gauze) to open wounds • Start appropriate ABX (Ancef +/- other depending on contamination), update tetanus
Ultimately, splint fractures/dislocations to prevent further displacement/soft tissue trauma and for comfort The following slides outline how to splint an injured patient awaiting orthopaedic assessment/for transport They do not necessarily represent the preferred method of definitive immobilization
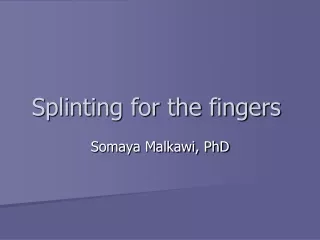
Sprains: buddy tape (padding in between, tape around distal phalanx only to allow more dynamic rehab) Fractures/Dislocations: padded malleable aluminum splint Fingers
Metacarpals • Buddy tape affected finger to adjacent normal finger, radial or ulnar gutter across MCP to PIP joint • Consider position of rest but avoid displacing fracture
For scaphoid (snuffbox) tenderness: thumb spica (OK sign) For other wrist sprains/dislocations/ carpal/metacarpal fractures: volar slab in position of function (holding a beer can) Carpals/Wrist
Both Bones mid diaphysis – forearm sugartong Prevents pro-supination Forearm
Distal humerus, radial head, olecranon fractures Collateral ligament strains Dislocations Posterior Slab Elbow
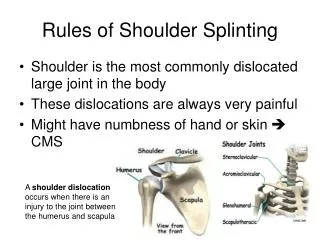
Proximal Humerus • Collar and Cuff for angulated/displaced proximal humerus fractures needing ligamentotaxis • Sleep upright in chair • Minimally displaced proximal humerus/ clavicle/AC jt. – Sling/Shoulder Immobilizer
Unstable pelvic fractures (open to AP compression or vertical shear) require a pelvic binder (bedsheet) – best placed at level of the greater trochanters Pelvis
Proximal femur (hip fractures) MAY symptomatically benefit from Buck’s traction (not necessary) Mid-shaft femur fractures require a Thomas Splint or Sager Splint for transport Femur
Femur Cont. • Sager Splint
Knee – ligamentous sprains, distal femoral/tibial plateau fractures: immobilization in extension Knee
Midshaft tibia/fibula fractures are best immobilized with a posterior slab (above knee) Ankle fractures should have medial and lateral support in addition to the posterior slab Tarsal fractures and toes: posterior slab (below knee) Below the Knee
Case 1 • 42 year old male (Mr. Griswold) is unloading his ATV from the back of a pickup • Riding off the bed, the ramp gives way and he sustains a FOOSH • He has wrist pain and deformity
Case 2 • His 43 year old wife (Mrs. Griswold) tries to run to his aid and trips on a root • She has a rotational injury to her ankle and is unable to weight bear • There is pain medially and laterally with swelling and deformity
Case 3 • Alarmed at the mayhem their 21 year old son (Gris Junior) runs to the cottage to call an ambulance • He too falls victim to a FOOSH • There is pain in the snuffbox of his hand
Case 4 • The petulant 15 year old Griswold daughter is furious that no-one can bring her for ice cream • She punches the ATV, full of spite and teen angst • She has pain along the ulnar border of her hand