Download
1 / 52
520 likes | 920 Vues
Peripheral Nerve Injuries of the Upper Limb. Stacy Rudnicki, MD Associate Professor of Neurology. Definitions. Radiculopathy. Process affecting the nerve root, most commonly by a herniated disc Weakness in muscles supplied by the nerve root (myotome)

E N D
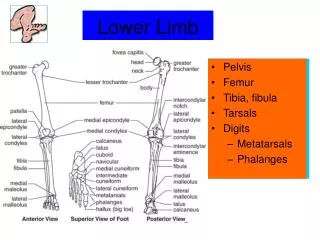
Peripheral Nerve Injuries of the Upper Limb Stacy Rudnicki, MD Associate Professor of Neurology
Radiculopathy • Process affecting the nerve root, most commonly by a herniated disc • Weakness in muscles supplied by the nerve root (myotome) • Sensory loss in the area of the skin supplied by the nerve root (dermatome)
Mononeuropathy • Dysfunction of a single peripheral nerve • Weakness in muscles supplied by the nerve • Sensory loss in the area of the skin supplied by the cutaneous branches of the nerve
Brachial Plexopathy • Can refer to involvement of the entire plexus, or parts of the plexus • Trunk lesion • Cord lesion • Distribution of weakness and numbness depends upon the part of the plexus affected
Sensory Supply to the Arm • Because fibers from different nerve roots come together and then split apart in the plexus • A dermatome may include areas of the skin supplied by different peripheral nerves • A single nerve may supply sensation to skin covered by more than one dermatome
Sensory Supply to the Arm • Because of the pattern of root contribution to the plexus: • An upper trunk lesion has sensory loss in the combined C5,6 dermatomes • A middle trunk lesion has sensory loss in the C7 dermatome • A lower trunk lesion has sensory loss in the combined C8T1 dermatomes
Principles of Localization • Certain sites are prone to nerve entrapments/injuries • Nerve opposing bone • Ulnar nerve at the elbow • Closed spaces • Carpal tunnel • Adjacent structures • Median nerve at the elbow, adjacent to the brachial artery
Principles of localization, cont • Order in which branches arise • Movements at specific joints • Single nerve • Elbow extension • Radial • Multiple nerves • Elbow flexion • Musculocutaneous • Radial • Thumb • Multiple different movement accomplished by multiple muscles innervated by the median, ulnar, and radial nerves
Work Back from the Exam • What muscles are weak? • What innervates the muscle? • Peripheral nerve • Part of plexus • Cord • Trunk • Nerve roots • Where is the sensory loss? Does it best follow the pattern of • A dermatome • A single nerve • A cord or trunk of the plexus
Case 1 • A 38 yo woman was the restrained passenger in a car struck head on • She braced her hands on the dashboard immediately prior to impact • She suffered bilateral fractures of the humerus at the spiral (radial) groove • She complains of diffuse aches in her arms and neck and weakness in her arms
Case 1, cont • On exam she has: • Bilateral wrist and finger drop (ie profound weakness of wrist and finger extension at the MCPs) • Weakness of supination • Weakness of elbow flexion with forearm held so that thumb is toward shoulder, but not with hand held in supination • Remainder of strength exam is normal • She has numbness in the posterior forearm extending into dorsum of hand into thumb and proximal index finger
Case 1, cont • FINDING MUSCLE ROOT PLEXUS P N WR DROP ECR, ECU C5,6,7,8 POST C RADIAL UT, MT, LT FING DRP EDC,EI C7, C8 POST C RADIAL MT, LT ELB FLX BR C5,C6 POST C RADIAL UT SENS ---- C6 Post C RADIAL UT
Triceps, long head Triceps, lateral head Triceps, med hd Brachioradialis ECRL ECRB Superficial Supinator Radial sens Ext Digit Abd Pol Longus Post Interosseous Ext Pol Longus Ext Pol Br Ext Indicies
Sensory loss in a high radial nerve lesion(Signficant variability b/w patients)
Final Diagnosis Bilateral radial nerve palsies at the spiral (radial) groove related to fractures
Case 2 • A 25 year old man gets involved in a fist fight and the police arrest him • When he is released on bail, he goes to see his doctor because he has numbness in the hand • On exam he had • a number of scratches and bruises on both arms • normal strength • sensory loss on the dorsum of the hand
Case 2, cont FINDING ROOT PLEXUS PN SENS LOSS < C6 < Post CORD SUP RAD SENS
Triceps, long head Triceps, lateral head Triceps, med hd Brachioradialis ECRL ECRB Superficial Supinator Radial sens Ext Digit Abd Pol Longus Post Interosseous Ext Pol Longus Ext Pol Br Ext Indicies
Final Diagnosis Superficial radial neuropathy secondary to handcuffs
Case 3 • 15 yo football player is hit be another player, with the helmet striking him in the axilla • On getting up, he is aware of shoulder weakness and pain and is taken to the ER
Case 3, cont • On exam he has: • Normal elbow flexion • Normal elbow extension • Normal shoulder adduction • Ability to initiate shoulder abduction, but he cannot raise his arm more than 15 degrees • Mild weakness of external (lateral) rotation of the arm • A patch of sensory loss over his upper arm
Case 3, cont FINDING MUSCLE ROOT PLEXUS PN Abd>15 Deltoid C5,6 Post C Axillary UT Ext Rot T. Minor C5,6 Post C Axillary Infrasp C5,6 UT Suprascap Sens ------- <C5 <POST C Axillary <UT
Case 3, cont • If it’s at the posterior cord • Radial innervated muscles should be affected • But elbow extension is spared • If it’s at the upper trunk • Musculocutaneous innervated muscles should be affected • But elbow flexion is spared • Pattern of sensory loss
Case 3, Final diagnosis Axillary Neuropathy
Case 4 • A 55 yo hospital worker comes to see you with a 2 week history of pain in her neck, shoulder, and upper arm • Symptoms began when she tried to help restrain a combative patient
Case 4, cont • On exam she she: • Weakness of shoulder abduction • Weakness of elbow flexion • Mild weakness of pronation • Sensory loss in her lateral forearm and thumb both posteriorly and anteriorly
Case 4, Final Diagnosis C6 Radiculopathy secondary to a herniated disc
Case 5 • 40 yo woman comes to see you because she has noticed weakness and numbness in her right hand • This started 2 months ago and is slowly worsening • She is otherwise healthy, and rides her bike at lease 40 miles per week
Case 5, cont • On exam she has: • Atrophy of the interosseous muscles of the right hand • Mild weakness of abducting and adducting the fingers • Normal thumb abduction, opposition and extension • Normal wrist flexion, abduction and adduction
Case 5, cont • If it’s the lower trunk, C8/T1, or medial cord other muscles affected should include: • APB and Opponens pollicus (median) • EPL and EPB (radial) But these muscles are spared
Ulnar sensory loss in an ulnar lesion proximal to the midforearm
Ulnar nerve Elbow Flexor carpi ulnaris Flex Dig Prof III/IV Dorsal uln cut Wrist Adductor Pollicus Abductor Flex Pollicus Br Opponens Digiti Minimi Flexor Dorsal/palmar Interosseous 3rd/4th lumbricals
Case 5, final diagnosis Ulnar neuropathy at the wrist
Case 6 • A 34 yo woman, currently 28 weeks pregnant, complains of numbness in her fingers • She finds that it is more difficult to manipulate small objects • She is awakened at night be tingling and pain in her hand which seems to spare her little finger
Case 6, cont • On exam she has: • Mild weakness of thumb abduction and opposition • Decreased pin prick on the palmar aspect of the thumb, index, middle and lateral aspect of the ring finger • Normal reflexes • No evidence of loss of muscle bulk in the hand
Case 6, cont Finding Muscle Root Plexus Nerve Thumb Abd APB C8, T1 Lower trunk Median Medial cord Thumb opp OP C8T1 Lower trunk Median Medial cord Sensory loss C6, 7 UT & LT Median Lateral cord
Case 6, cont Final Diagnosis Carpal tunnel syndrome (median neuropathy at the wrist)
Case 7 • This 38 yo man fell off a ladder and acutely noted weakness in his right arm • He suffered a fracture of his right clavicle • He c/o pain in the shoulder
Case 7, cont • His exam shows: • Weakness of initiating abduction of his right arm • If you raise his right arm to 90 degrees, he is unable to maintain it • With his arm at his side, he is unable to turn his forearm back • Weakess of elbow flexion • Numbness of the lateral arm and forearm
Case 7, cont Finding Muscle Root Plexus Nerve 1 sh abd Supraspinatus C5,6 UT Suprascap 2 sh abd Deltoid C5,6 UT Axillary Post Cord Ext rot Infraspinatus C5,6 UT Suprascap Teres minor C5,6 UT, PC Axillary Elbow flexion Biceps C5,6 UT, LC Musc BR C5,6 UT, PC Radial Sensory C5 & 6 UT Axillary & LC & PC Musc
Case 7, cont • Since the suprascapular nerve is involved, must be at the level of the upper trunk or nerve root • Difficult to distinguish based on exam alone if this is upper trunk or C5 and C6 radiculopathies • Brachial plexopathies may occur with fractures of the clavicle • Radiculopathies are unusual without neck pain • Preservation of the function of serratus anterior muscle makes root less likely • Further studies (EMG) can help localize b/w root and trunk