Download
1 / 37
380 likes | 739 Vues
New Treatments for Sinus Disease. San Francisco Otolaryngology Medical Group David Schindler, Brian Schindler, Jacob Johnson, Andrea Yeung, Theresa Kim. Definition – Rhinosinusitis . A group of disorders characterized by inflammation of the mucosa of the nose and paranasal sinuses.

E N D
New Treatments for Sinus Disease San Francisco Otolaryngology Medical Group David Schindler, Brian Schindler, Jacob Johnson, Andrea Yeung, Theresa Kim
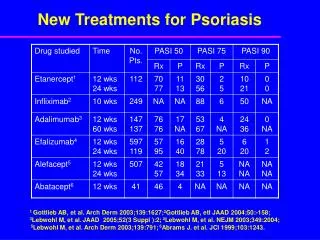
Definition – Rhinosinusitis A group of disorders characterized by inflammation of the mucosa of the nose and paranasal sinuses Reported Factors - Major • Mucopurulent drainage (anterior or posterior) • Nasal obstruction (congestion) • Facial pain-pressure fullness • Decreased sense of smell Additional Examination • Nasal Endoscopy • Purulence • Edema, erythema • Polyps • CT imaging • Allergy and immune testing “Clinical practice guideline: Adult sinusitis” Rosenfeld et al., Otolaryngology–Head and Neck Surgery (2007) 137, S1-S31
Rhinosinusitis Disease Progression Increasing symptom duration & frequency Acute Subacute Recurrent Chronic • Up to 4 weeks in duration • Purulent nasal discharge and/or • Nasal obstruction • Facial pain-pressure-fullness • 4-12 Weeks in duration • Symptoms as in acute disease • 4+ episodes/yr, 10+ days in duration or worsening symptoms within 10 days of onset • Symptoms as in acute disease • 12+ weeks in duration • 2+ symptoms • Mucopurulent drainage • Nasal Obstruction • Facial Pain-pressure-fullness • Decreased sense of smell • Pathology evident on endoscopic or CT examination “Clinical practice guideline: Adult sinusitis” Rosenfeld et al., Otolaryngology–Head and Neck Surgery (2007) 137, S1-S31
Rhinosinusitis Disease Model Natural Mucociliary Transport and Drainage Bony Scaffold Mucosal Surface Bone and tissue structure enable natural sinus clearance Multiple factors can impair mucociliary clearance, hindering or stopping normal drainage of the sinuses Anatomic Factors Microbial Factors Acute Sinusitis Allergic Factors Immune Factors Chronic Sinusitis/ Recurrent Acute Sinusitis Acute sinusitis can progress to a recurrent or chronic disease state Although medical management is adequate for ~80-90%1of patients; recalcitrant disease may require surgical treatment 1. Data on file
Sinusitis is a medical disease until ostial restriction cannot be reversed by medical treatment Surgical Intervention in Disease Progression Anatomy- Filtering system Allergy/ Inflammation Immune Sinus Drainage
2 Weeks Later, No Treatment Acute Viral URI Coronal CT Scans for Rhinosinusitis • Indicated for: • questions of diagnosis &/or therapy • strong history & not responding to therapy • extrasinus spread of infection • in chronic RS, after 4 weeks or more of appropriate therapy • prior to sinus surgery • Timing of CT scan • Note in acute viral URIs that 87% of sinus CTs are positive, & 21% remain so 2 weeks after clinical resolution Source: Gwaltney J, et al. N Engl J Med 1994;330:25–30.
XoranMiniCAT CT Scanner 10-40 secondsOnline access for outside providersIndependent review from outside radiology0.04-0.17 msv of radiation vs 2msv in traditional CT sinus
What are the goals of Sinus Surgery? • Open blocked ostia to restore ventilation and to restore normal sinus function • Allows drainage and reversal of mucosal disease • Preserve as much normal anatomy and mucosa as possible • Promotes faster healing • Reduces the inflammatory response • Improves surgical outcomes
Sinus surgery has continued to evolve over time 90 years 20 years • The advent of FESS in 1985 allowed for sinus surgery without traumatic trans-antral penetration or inferior antrostomies1 • Recent advances in instrumentation enable ENT surgeons to perform FESS without traumatic bone resection or mucosal stripping • Drainage via natural ostia can be restored in a minimally-invasive manner2 1893 - 1985 1985 - 2005 2005 - Present Caldwell-Luc Antrostomy Functional Endoscopic Sinus Surgery (FESS) FESS w/ balloon catheters 1 2 1. DW Kennedy, “Functional Endoscopic Sinus Surgery” Arch Otolaryngol. 1985;111(10):643-649. 2. Weiss et. Al, “Safety and outcomes of balloon catheter sinusotomy: A multicenter 24-week analysis in 115 patients” Otolaryngology-Head and Neck Surgery (2007) 137, 10-20
History – Sinus surgery prior to 1985 Caldwell-Luc Antrostomy Intranasal Ethmoidectomy Inferior Antrostomy Prior to the advent of FESS, sinus surgery was highly disruptive to natural structures in the face and nasal cavity
Functional Endoscopic Sinus Surgery 1. Trans-nasal approach 2. More precise instrumentation 3. Image-guided navigation • Nasal approach reduces structural trauma • Microdebriders enable a more targeted dissection/resection process • Image guidance reduces uncertainty during approach to treatment site FESS significantly reduced the invasiveness of sinus surgery, and it continues to evolve today
The paradox between the goals and the application of Functional Endoscopic Sinus Surgery • First goal, to open blocked sinuses, is usually achieved at the expense of • The second goal, the preservation of normal anatomy and mucosa. • The flexible instruments of the balloon technology platform provide tools designed to navigate the complex paranasal anatomy and to achieve ostial dilation with minimal intervention . • Preserving the filtering function of the nose.
FESS & Balloon Catheter Cost in OR 1 2 Average Hospital Charges Balloon catheter devices (with balloon): $1,500 Microdebrider and blades (without balloon): $500 C-arm fluoroscopy (with balloon): $750 Image-guidance (without balloon): $500 OR time: $600 per 15 min PACU time: $300 per 15 min Friedman M, et al., Functional Endoscopic Dilatation of the Sinuses: Safety, Feasibility, Patient Satisfaction and Cost Am J Rhinol 2008; 22:204–9.
Balloon Catheter Cost in OR vs. in Office **Other includes the cost related to OR treatment for cross-over patients.
Current in Office Sinus Procedures Office procedures to understand/ influence anatomy: • Endoscopy • CT sinus • Proetz sinus displacement • Maxillary sinus tap • Office Sinuplasty/ sinus lavage • Inferior Turbinate reduction • Nasal Polypectomy
Office Sinuplasty/ Sinus Lavage • Patient Selection and Tolerance Access sinus cavity Dilate natural ostium Directly irrigate sinus Remove system
Patient Selection – Typical profiles • Chronic maxillary, frontal, sphenoid sinusitis • Revision cases with scarring. Incomplete outflow tract obstruction • Chronic sinusitis with need for lavage • Avoid: • Cases with extremely complex anatomy, complete scar occlusion, etc • Cases requiring significant ancillary procedures (e.g. turbinectomy, septoplasty) • Patients with anxiety, claustrophobia, low pain threshold
Patient Selection OR Office • Patient Motivation • Cash pay patients • Primary vs. Revision Cases • Anesthesia concerns • Patient Tolerance • Dental procedure tolerance • Patient Anatomy • Deviated Nasal Septum (3 mm) • Inferior Turbinate • Uncinate Process • Ethmoid Bulla • Nasal Polyps • Middle Turbinate: Scar bands, Lateralized Middle Turbinate, Concha Bullosa • Image guidance • Patient General Health • Monitoring, Bleeding, Cardio-pulmonary status, Cough
Sino-nasal Innveration Nerve Block for Local Anesthesia • Anesthesia Options • Oral (valium, optional) • Sprays (pontocaine, ephedrine 1%, afrin) • Injection (lidocaine with epinephrine 7mg/kg) • Nerve block (ethmoid, sphenopalatine) Spheno- palatine Block Anterior Ethmoid Block
Operating Room vs. In-Office Study Tolerability Rating 95% of respondents rated in-office procedure as tolerable or better Highly tolerable Not tolerated
Operating Room vs. In-Office Study Pain Rating • 70% reported pain as Low Intensity (0-2) during balloon inflation • No correlation between type of local anesthetic used and pain level Intense Pain No Pain
6 months 1 year 40 weeks 2 years Multicenter registry confirms findings of CLEAR 24 week, 1 and 2 year studies CLEAR Study PatiENT Registry No serious adverse events No serious adverse events Safety 91.6% patency @ 1 yr 2.4% patient revision rate Efficacy Patient Satisfaction SNOT-20 Score -1.30 @ 2 yr (1) 95.2% symptom improvement Levine, HL, et al, “Multicenter Registry of Balloon Catheter Sinusotomy Outcomes for 1,036 Patients.” Annals of Otology, Rhinology & Laryngology. April 2008; Vol. 117(4): 263-270.
The Old and the New – Paradigm shift Successful post-sinuplasty “big hole surgery”
Summary • In a small percentage of patients, rhinosinusitis becomes a recurrent or chronic disease which is refractory to medical management. • There has been an evolution of sinus procedures to improve sinus drainage in medically refractory rhinosinusitis. • Functional Endoscopic Sinus Surgery (FESS) has advanced the management of chronic rhinosinusitis. • Current research is exploring the limitations of traditional rigid instrumentation in FESS. • FESS with balloon catheters offers a minimally-invasive way to achieve classic sinus surgery goals. • Balloon catheters and other office based procedures are now available to improve medically refractory rhinosinusitis.
Case 1: Acute Dental Rhinosinusitis 81 yo female with L acute face pain and yellow dc after dental procedure Immune: Anaerobic infection (PCN allergy) Allergy: Pollen Structure: Dental implant Plan: L maxillary sinuplasty, Clindamycin and removal of implant
Case 1 Pearls * Avoid sinusitis complications * Avoid anesthesia complications * PCN allergy & dental issues
Case 2: Fungal Sinusitis 83 yo female with Crohn’s disease and on Coumadin for coronary issues Kenneth D Faw MD Everen Sinus Center
Mycetoma Endoscopic Case 2 Kenneth D Faw MD Evergreen Sinus Center
Case 2 Pearls * Calcifications on CT
Case 3: Revision L Frontal and R Sphenoid Sinus KD, 2/26/09 KD, 7/27/09
Case 3 Pearls * Post op care and need for revisions -avoid surgery complications and take backs