Download
1 / 1
10 likes | 138 Vues

E N D
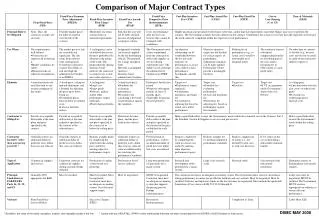
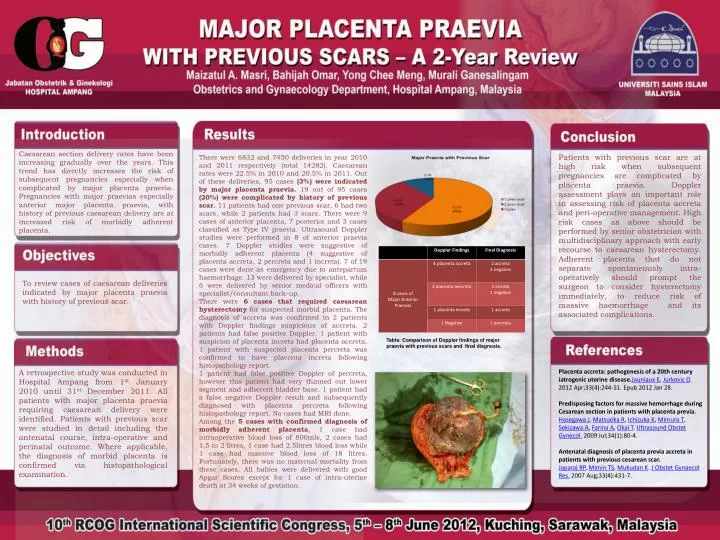
Patients with previous scar are at high risk when subsequent pregnancies are complicated by placenta praevia. Doppler assessment plays an important role in assessing risk of placenta accreta and peri-operative management. High risk cases as above should be performed by senior obstetrician with multidisciplinary approach with early recourse to caesarean hysterectomy. Adherent placenta that do not separate spontaneously intra-operatively should prompt the surgeon to consider hysterectomy immediately, to reduce risk of massive haemorrhage and its associated complications. Caesarean section delivery rates have been increasing gradually over the years. This trend has directly increases the risk of subsequent pregnancies especially when complicated by major placenta praevia. Pregnancies with major praevias especially anterior major placenta praevia, with history of previous caesarean delivery are at increased risk of morbidly adherent placenta. There were 6832 and 7450 deliveries in year 2010 and 2011 respectively (total 14282). Caesarean rates were 22.5% in 2010 and 20.5% in 2011. Out of these deliveries, 95 cases (3%) were indicated by major placenta praevia. 19 out of 95 cases (20%) were complicated by history of previous scar. 11 patients had one previous scar, 6 had two scars, while 2 patients had 3 scars. There were 9 cases of anterior placenta, 7 posterior and 3 cases classified as Type IV praevia. Ultrasound Doppler studies were performed in 8 of anterior praevia cases. 7 Doppler studies were suggestive of morbidly adherent placenta (4 suggestive of placenta accreta, 2 percreta and 1 increta). 7 of 19 cases were done as emergency due to antepartum haemorrhage. 13 were delivered by specialist, while 6 were delivered by senior medical officers with specialist/consultant back-up. There were 6 cases that required caesarean hysterectomy for suspected morbid placenta. The diagnosis of accreta was confirmed in 2 patients with Doppler findings suspicious of accreta. 2 patients had false positive Doppler. 1 patient with suspicion of placenta increta had placenta accreta. 1 patient with suspected placenta percreta was confirmed to have placenta increta following histopathology report. 1 patient had false positive Doppler of percreta, however this patient had very thinned out lower segment and adherent bladder base. 1 patient had a false negative Doppler result and subsequently diagnosed with placenta percreta following histopathology report. No cases had MRI done. Among the 5 cases with confirmed diagnosis of morbidly adherent placenta, 1 case had intraoperative blood loss of 800mls, 2 cases had 1.5 to 2 litres, 1 case had 2.5litres blood loss while 1 case had massive blood loss of 18 litres. Fortunately, there was no maternal mortality from these cases. All babies were delivered with good Apgar Scores except for 1 case of intra-uterine death at 34 weeks of gestation. To review cases of caesarean deliveries indicated by major placenta praevia with history of previous scar. Table: Comparison of Doppler findings of major praevia with previous scars and final diagnosis. Placenta accreta: pathogenesis of a 20th century iatrogenic uterine disease.Jauniaux E, Jurkovic D. 2012 Apr;33(4):244-51. Epub 2012 Jan 28. Predisposing factors for massive hemorrhage during Cesarean section in patients with placenta previa. Hasegawa J, Matsuoka R, Ichizuka K, Mimura T, Sekizawa A, Farina A, Okai T. Ultrasound Obstet Gynecol. 2009 Jul;34(1):80-4. Antenatal diagnosis of placenta previa accreta in patients with previous cesarean scar. Japaraj RP, Mimin TS, Mukudan K. J Obstet Gynaecol Res. 2007 Aug;33(4):431-7. A retrospective study was conducted in Hospital Ampang from 1st January 2010 until 31st December 2011. All patients with major placenta praevia requiring caesarean delivery were identified. Patients with previous scar were studied in detail including the antenatal course, intra-operative and perinatal outcome. Where applicable, the diagnosis of morbid placenta is confirmed via histopathological examination.