Download
1 / 12
120 likes | 128 Vues
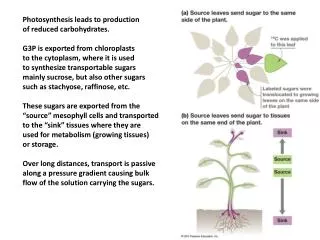
Show Me the Sugars!. Grady Health System, International Medical Clinic. Sol Aldrete, MD, Roger Alvarez, DO, Jeremy Chow, MD, Juan Ortega-Legaspi, MD, Lori Randall, MD, Amy Salerno, MD, Danny Treiyer, MD, Aida Venado, MD Faculty Mentor: Nurcan Ilksoy. Tests of Change. Problem. Measure.

E N D
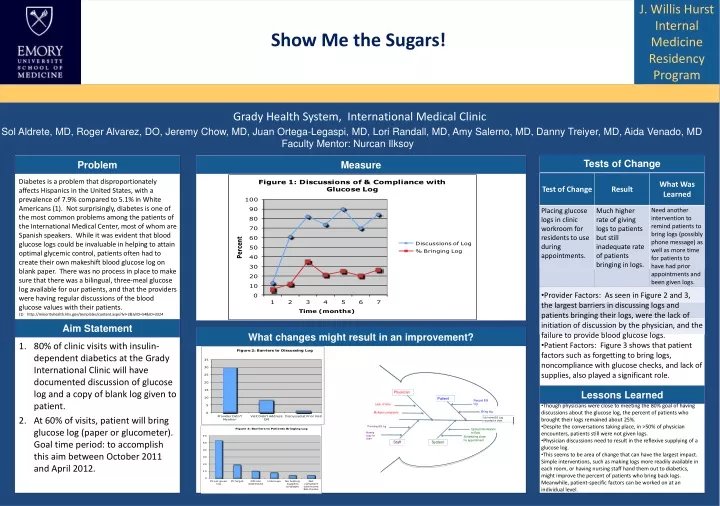
Show Me the Sugars! Grady Health System, International Medical Clinic Sol Aldrete, MD, Roger Alvarez, DO, Jeremy Chow, MD, Juan Ortega-Legaspi, MD, Lori Randall, MD, Amy Salerno, MD, Danny Treiyer, MD, Aida Venado, MD Faculty Mentor: Nurcan Ilksoy Tests of Change Problem Measure Diabetes is a problem that disproportionately affects Hispanics in the United States, with a prevalence of 7.9% compared to 5.1% in White Americans (1). Not surprisingly, diabetes is one of the most common problems among the patients of the International Medical Center, most of whom are Spanish speakers. While it was evident that blood glucose logs could be invaluable in helping to attain optimal glycemic control, patients often had to create their own makeshift blood glucose log on blank paper. There was no process in place to make sure that there was a bilingual, three-meal glucose log available for our patients, and that the providers were having regular discussions of the blood glucose values with their patients. (1) http://minorityhealth.hhs.gov/templates/content.aspx?lvl=2&lvlID=54&ID=3324 Barriers • Provider Factors: As seen in Figure 2 and 3, the largest barriers in discussing logs and patients bringing their logs, were the lack of initiation of discussion by the physician, and the failure to provide blood glucose logs. • Patient Factors: Figure 3 shows that patient factors such as forgetting to bring logs, noncompliance with glucose checks, and lack of supplies, also played a significant role. Aim Statement What changes might result in an improvement? • 80% of clinic visits with insulin-dependent diabetics at the Grady International Clinic will have documented discussion of glucose log and a copy of blank log given to patient. • At 60% of visits, patient will bring glucose log (paper or glucometer). Goal time period: to accomplish this aim between October 2011 and April 2012. Lessons Learned Physician Patient Record BG log • Though physicians were close to meeting the 80% goal of having discussions about the glucose log, the percent of patients who brought their logs remained about 25%. • Despite the conversations taking place, in >50% of physician encounters, patients still were not given logs. • Physician discussions need to result in the reflexive supplying of a glucose log. • This seems to be area of change that can have the largest impact. Simple interventions, such as making logs more readily available in each room, or having nursing staff hand them out to diabetics, might improve the percent of patients who bring back logs. Meanwhile, patient-specific factors can be worked on at an individual level. Lack of time Multiple complaints Bring log No home BG Log recorded in chart Providing BG log Upload information to Epic Making copy for chart Scheduling close f/u appointment Staff System
End-of-Life Care PlanningImproving Documentation of Advanced Directives in the Resident Clinic using Electronic Medical Records Grady Primary Care Center, Monday Purple Pod Salim Hayek, Ria Nieva, Frank Corrigan, Amy Zhou, Uma Mudaliar, David Mays, Michael Massoomi, Erika Heard, Reza Hassanyar, Dejuan White Faculty Mentors: Iris Castro, Nurcan Ilksoy Tests of Change Problem Methods and Measure • End-of-life care planning has received and advocacy in recent years. JCAHO requires that hospital medical records document evidence of known advanced directives (AD) and provide information about advance care planning to all patients. Patient satisfaction is increased when AD are discussed in clinic. • Despite surveys showing patients prefer to discuss advance directives with their primary care doctor, many are completed during hospitalizations. Population based-estimates of completed advance directives range from 5% to 15%. • Discussing end-of-life care in the outpatient setting is perceived as challenging. One major obstacle reported by physicians is lack of time and effective reminders to address and document advanced directives. Yes No • A total of 588 patient charts were screened by 7 providers of Grady Clinics Purple Pod. • 157 met the predefined criteria for AD documentation. • “Advanced Directives Counseling” was added to the problem list of 50% of patients who met criteria. • During the period of November 2011-April 2012; 64 patients were seen in clinic; 38 had AD on their problem list, 26 did not. • 76% of charts with ADPL had documentation of AD. Only 11.5% of those without ADPL had AD documented. Limitations • Sample size was relatively small and study of short duration. Will require longer term and larger population sample to assess sustainability of the improvement in documentation rate. • Study does not assess completion rates of official AD document completion. • No conclusion can be made on the impact of improved AD documentation on inpatient management TOC1 TOC2 TOC3 Data Collection Aim Statement Barriers to Documentation of Advanced Directives • Previously we assessed the effectiveness of email-mediated provider education and reminders in improving documentation of AD. This initial test of change (TOC1) showed a slight (1%) and temporary increase in documentation of AD. • Using the electronic medical records (EMR) system EPIC we set to implement a reminder system for physicians to document AD in a select population of patients with chronic illnesses (see below), and assess the percentage of patients meeting criteria which have documented AD counseling within 6 months of the main test change: • Adding “Advanced Directives Counseling” to the patient problem list (ADPL). • Patients must have one or more of the following characteristics/diagnoses: Age > 65, Congestive Heart Failure NYHA III, severe COPD (FEV1<30%), AIDS, any diagnosis of malignancy, cirrhosis, ESRD, stroke. Lessons Learned • EMR based reminders are effective in improving documentation rates of AD and may be applied for other purposes. • Obstacles remain, including the lack physicians’ initiative and knowledge in discussing AD, time limitations in the outpatient setting, as well as the unclear translation into changes in inpatient management. • Further research is needed to establish the sustainability of improved documentation over longer periods of time and in a larger population sample, as well as its impact on inpatient management.
Improving Influenza Vaccination Rates in an Internal Medicine Resident Clinic General Internal Medicine at 1525 Clifton Rd., Friday Resident Clinic Turang Behbahani, Vivian Cheng, Ed Clermont, Tina Constantin, Patrick Hall, Farah Khan, Freny Nirappil, Julian Raffoul, Nathan Spell Barriers Problem Measure The number of seasonal influenza-associated deaths varies from year to year because flu seasons are unpredictable and often fluctuate in length and severity. The CDC estimates that from the 1976-1977 season to the 2006-2007 flu season, flu-associated deaths ranged from a low of about 3,000 to a high of about 49,000 people (1). In 2013, the CDC published a model to quantify the annual number of influenza-associated illnesses and hospitalizations averted by influenza vaccination during the 2006–11 influenza seasons (2). Using that model the CDC estimated that vaccination resulted in 79,000 (17%) fewer hospitalizations during the 2012–13 influenza season than otherwise might have occurred. Especially in the primary care setting, providers are facing increasing difficulties to clarify "influenza-myths" as well as to identify burdens which keep patients from choosing or receiving the valuable vaccination. • Lack of a standard process to address preventive care, in general, leading to creation of unique solutions to this problem • Perceived inability to influence patient wishes and misinformation • Relative little involvement of clinic staff Goal Actual Lessons Learned Standard process Attd review • Doing an improvement project in isolation from the rest of the practice made it hard to create a standard way of checking vaccine status that would sustain itself • A standard process does not become the standard without effective training and reinforcement at first • Reliance on memory does not yield much improvement • We tended to make changes where we felt we had the most control, rather than trying to change patient beliefs, which was the greatest opportunity • Data collection should be built into the work flow or should come from a ready source What changes might result in an improvement? Aim Statement By January 1, 2014, 70% of more of all patients seen in the Friday resident clinic at 1525 Clifton Road will be vaccinated during their appointment (if not already completed). References Tests of Change (1) Thompson MG et al., Estimated Deaths Associated with Seasonal Influenza - United states 1976-2006, Weekly, August 27, 2010 / 59(33);1057-1062 (2) CDC. Prevention and control of seasonal influenza with vaccines. Recommendations of the Advisory Committee on Immunization Practices—United States, 2013–2014. MMWR 2013;62(No. RR-7). • Jan: Created standard process to let MD know patient’s status and wishes • Feb: Attending to review vaccine status during sign-out as detection and mitigation step.
Improving Hypertension Control in the Patient Centered Medical Home Grady Green Pod Clinic Team Austin Chan, Maya Varthi, N. Thi Gunter, Patricia Hwang, Curtis Jamison, Bryant Chan, Arjun Nanda, Jessica Nave, Ravi Vora, Parth Joshi, Mahmoud Abdou, Danesh Kella, Greg Weston, Amirali Masoumi, Abhinav Koul, Abdullah Khan, Bradley Witbrodt, James Monaco, Vaishnavi Kundel, Yasamin Chowdhury, Danny Nguyen, Maria Lee, Anjan Deka, Phoebe Chi, Eric Shin, Aaron Gluth, Brian Heeke, Sandeep Krishnan, Anand Jain, Daniel Cucco, Vera Tate, Ula Abed Alwahab, Neal Bhatia, Kiran Valiani, Akshay Shetty, Shing-Yu “Cliff” Lin, Sara Turbow, Teresa Ingram, Katie Tipton, Robert McClung, David Dunhill, Valeria Cantos-Lucio, Joy Wortham, Shadi Yarandi, Nisha Joseph, Taylor Lebeis Faculty Mentors: Kalra, Girish L; Doyle, Joyce P; Bussey-Jones, Jada; Manning, Kimberly; Jones, Danielle; Schneider, Jason S; Adhyaru, Bhavin; Ilksoy, Nurcan Green Pod Nurses and Staff Tests of Change Problem What changes might result in an improvement? • Dec - To improve the accuracy of BP measurement and better identify patients who require intensification, at each visit, a manual BP is repeated in patients who are hypertensive, the physician is notified, and the value is recorded within the EMR. • Feb – To improve patient adherence, the remark “For High Blood Pressure” is added to the sig line of prescriptions for antihypertensives. • Mar – Within our Epic EMR, a “dot phrase” reminder is added to the primary clinic note template that prompts physicians to address HTN. In our urban primary care center, a disproportionately large percentage of patients have uncontrolled hypertension compared to the general population. Moreover, among academic primary care clinics within the Grady Memorial Hospital Primary Care Center, a recent report revealed that our Green Pod practice ranked last in blood pressure control. In 3648 Green Pod patient encounters in June 2012, only 57.2% had a SBP < 140 mmHg, compared to 65.2%, 65.4%, and 70.4% in the Orange Pod, Purple Pod, and Yellow Pod clinics, respectively. We sought to re-design our approach to hypertension management by identifying reasons for poor blood pressure control and devising interventions to help us more successfully treat our patients. Figure 1. Fishbone diagram addressing barriers to effective BP control. Three key barriers were addressed in our study: one physician factor, one nursing factor, and one patient-related factor. Additional Pitfalls Additional barriers contributing to suboptimal blood pressure control and possible decreased effectiveness of our interventions included: Erratic participation by providers Time constraints within a busy primary care clinic Patient resistance to the addition of medication and physician uneasiness with intensifying therapy in the setting of possible non-adherence. Limited patient finances and possible low literacy. Measure Figure 2. Percentage of return patients with SBP < 140 mmHg Among patients who have been seen in the clinic 2 or more times in the preceding six months, the percentage of visits with a systolic BP < 140 mmHg. n = return visits examined among Green, Orange, and Purple clinics. Note that these figures should not be compared to the percentages cited from the June 2012 report, which examined all patients. Aim Statement Lessons Learned Over 6 months, we aim to increase the percentage of Green Pod patients with hypertension who meet a systolic blood pressure goal of < 140 mm Hg to over 70%. • Three simple, low-cost interventions showed varying degrees of benefit in helping our patients achieve BP control. • Utilizing support staff in the clinic appeared to be the most effective intervention, though the practice of preferentially obtaining manual BP assessments when the initial automated reading is high likely introduced some bias. • We were only partially able account for patients who were uncontrolled and then had meds changed. • Ensuring physician participation in a busy clinic setting without providing additional incentive was challenging. Baseline TOC #1 TOC #2 TOC #3 n = 292 n = 320 n = 268 n = 516 n = 594 n = 599
Improving Hepatitis C Screening in a Primary Care Internal Medicine Resident Clinic 1525 Clifton Road Emory Clinic Friday Team FrenyNirappil MD, Vivian Cheng MD, Tina Constantin MD, Edward Clermont MD, Patrick Hall MD, Michael Lava MD, Rachel Anquez MD Faculty Advisor: Nathan Spell III MD Test of Change #2 Test of Change # 2 Tally Sheet Fishbone Diagram
Improving Counseling for Tobacco Cessation in a Resident Primary Care Clinic Grady Primary Care Center, Friday Purple Pod Jane Titterington, Robert Kung, Zahi Mitri, Jeff Chen, Kyle James, Jenna Kay, Wendy Neveu, Reema Dbouk, Anthony Gamboa, Faculty Mentors: Sanjukta Chatterjee, Nurcan Ilksoy Problem and Background Outcomes Barriers • Cigarette smoking is the leading preventable cause of mortality in the United States, responsible for over 400,000 deaths annually1. • Up to one-half of all tobacco users can be expected to die from a tobacco-related disease2. • The economic burden of tobacco use is estimated to be $197 billion per year1. • Smoking cessation is associated with clear health benefits and should be a major health care goal3. • Screening all patients for tobacco use and providing all smokers a brief smoking cessation intervention is one of the three most cost-saving clinical preventive services3. • Less than half of all patients (48.7%) report receiving advice from health professionals to quit 4. • Most common physician barriers were: forgetting to address smoking status, not having enough time to address it or having too many other active medical problems to address, or failure to document in the progress note that tobacco cessation counseling occurred. • Lack of patient education materials was also a barrier to proper counseling. • RN barriers included lack of documentation of screening for tobacco use during triage, as well as having patients roomed before triage could occur. Test of Change #1 Test of Change #2 and #3 Lessons Learned • Screening for tobacco use by clinic nurses increased when incorporated into routine triage procedures. • Tobacco cessation counseling occurred significantly more frequently when providers were prompted by a standardized progress note template. Documentation of intervention was also more likely to be completed. • Having patient education materials readily available appeared to promote tobacco cessation counseling by providers, and ensured patients left clinic with specific resources to help them quit smoking. What changes might result in an improvement? Aim Statement Fishbone Diagram 1. We aim to screen 100% of our Friday Purple Pod patients for current tobacco use with corresponding documentation in EPIC by January 2012. 2. We aim to improve tobacco cessation counseling rates to greater than 80% of our population of current smokers, as measured by both documentation in clinic notes; as well as by including tobacco cessation resources in the patient’s after visit summary by May 2012. Tired of counseling Other more urgent concerns Not disclosing smoking status Only wants treatment Lack of time Forgets to discuss Forgets to document Other more urgent issues Physician Patient Counseling Prior status not updated Lack of counseling materials References No template in Epic Not documented Hospital System Not triaged Not in problem list in Epic Ancillary Staff (1) MMWR Morb Mortal Wkly Rep. 2008 Nov 14;57(45):1226-8. (2) http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf (3) Maciosek MV et al. Am J Prev Med 2006; 31:52. (4) MMWR Morb Mortal Wkly Rep. 2011 Nov 11;60(44):1513-9.
Improving the Documentation and Interventions of Obesity in a Resident Primary Care Clinic Grady Primary Care Center, Monday OrangePod Kobina Wilmot MD, Justin Cheeley MD, Jessie Torgerson MD, Jia Shen MD, Anita Saraf MD, Jenny Luke MD, Meena Prasad MD, Thomas Runge MD, Arash Harzand MD, Hassan Imam MD, Jessica McDermott MD, Faculty Mentors: Jada Bussey-Jones MD, Stacie Schmidt MD ,Nurcan Ilksoy MD Tests of Change Problem Measure • Obesity is defined as a BMI of >30. • More than 1/3 (35.7%) of U.S. adults are obese. The rate in Fulton County is 23.2%, in Dekalb County 27.4%. • Obesity is an increasing problem. Currently, >30% of the population is obese in 12 states. In 2000, no state had an obesity rate >30%. • The average hospital length of stay for obese patients is 60% longer than for normal weight individuals nationwide. • The annual cost of obesity in Georgia is $2.4 billion (or $250 per Georgian each year), including direct health care costs and lost productivity. • Obesity places patients at greater risk for diabetes, heart disease and some types of cancer. It is the #2 cause of preventable death in the United States. • After increasing obesity documentation in our clinic last year, we noted that despite documentation, interventions were often not addressed. The obesity clinic instituted by Dr. Schmidt became an additional resource to obese patients this year, in addition to nutrition classes and diet/exercise education by the health care practitioner. Barriers • Making BMI more visible in EMR • Time for physicians to make and offer specific education on diet and exercise • Assuring patients who are referred to obesity clinic have message sent to and received by clinic scheduler • Patients referred to obesity clinic actually are able to be reached to attend sessions • Enough sessions are available to accommodate the large number of obese patients in our primary clinic What changes might result in an improvement? Process Improvement Chart with possible interventions for improvement of outcome Lessons Learned • EMR has facilitated BMI as being listed as part of a patient’s vital signs for each visit, helping to prompt a response for an abnormal BMI • Though BMI is automatically calculated in EMR, obesity is still often overlooked by providers as a separate medical problem • If obesity is listed as a separate problem, an intervention is often proposed • Nutrition and obesity clinic referrals offer concrete actions providers can take to address obesity. Diet and education handouts may be helpful for providers to more readily access. Aim Statement We aim : • To continue to improve documentation of BMI in problem list to 75% by March 2012. • To have at least 50% of patients documented with obesity (BMI >30) to have an intervention of exercise, diet, or obesity referral by March 2012 in Orange Pod Monday clinic.
End-of-Life Care PlanningImproving Documentation of Advanced Directives in the Resident Clinic using Electronic Medical Records Grady Primary Care Center, Monday Purple Pod Salim Hayek, Ria Nieva, Frank Corrigan, Amy Zhou, Uma Mudaliar, David Mays, Michael Massoomi, Erika Heard, Reza Hassanyar, Dejuan White Faculty Mentors: Iris Castro, Nurcan Ilksoy Tests of Change Problem Methods and Measure • End-of-life care planning has received and advocacy in recent years. JCAHO requires that hospital medical records document evidence of known advanced directives (AD) and provide information about advance care planning to all patients. Patient satisfaction is increased when AD are discussed in clinic. • Despite surveys showing patients prefer to discuss advance directives with their primary care doctor, many are completed during hospitalizations. Population based-estimates of completed advance directives range from 5% to 15%. • Discussing end-of-life care in the outpatient setting is perceived as challenging. One major obstacle reported by physicians is lack of time and effective reminders to address and document advanced directives. Yes No • A total of 588 patient charts were screened by 7 providers of Grady Clinics Purple Pod. • 157 met the predefined criteria for AD documentation. • “Advanced Directives Counseling” was added to the problem list of 50% of patients who met criteria. • During the period of November 2011-April 2012; 64 patients were seen in clinic; 38 had AD on their problem list, 26 did not. • 76% of charts with ADPL had documentation of AD. Only 11.5% of those without ADPL had AD documented. Limitations • Sample size was relatively small and study of short duration. Will require longer term and larger population sample to assess sustainability of the improvement in documentation rate. • Study does not assess completion rates of official AD document completion. • No conclusion can be made on the impact of improved AD documentation on inpatient management TOC1 TOC2 TOC3 Data Collection Aim Statement Barriers to Documentation of Advanced Directives • Previously we assessed the effectiveness of email-mediated provider education and reminders in improving documentation of AD. This initial test of change (TOC1) showed a slight (1%) and temporary increase in documentation of AD. • Using the electronic medical records (EMR) system EPIC we set to implement a reminder system for physicians to document AD in a select population of patients with chronic illnesses (see below), and assess the percentage of patients meeting criteria which have documented AD counseling within 6 months of the main test change: • Adding “Advanced Directives Counseling” to the patient problem list (ADPL). • Patients must have one or more of the following characteristics/diagnoses: Age > 65, Congestive Heart Failure NYHA III, severe COPD (FEV1<30%), AIDS, any diagnosis of malignancy, cirrhosis, ESRD, stroke. Lessons Learned • EMR based reminders are effective in improving documentation rates of AD and may be applied for other purposes. • Obstacles remain, including the lack physicians’ initiative and knowledge in discussing AD, time limitations in the outpatient setting, as well as the unclear translation into changes in inpatient management. • Further research is needed to establish the sustainability of improved documentation over longer periods of time and in a larger population sample, as well as its impact on inpatient management.
Improving Influenza Vaccination Rates in an Internal Medicine Resident Clinic General Internal Medicine at 1525 Clifton Rd., Friday Resident Clinic Turang Behbahani, Vivian Cheng, Ed Clermont, Tina Constantin, Patrick Hall, Farah Khan, Freny Nirappil, Julian Raffoul, Nathan Spell Barriers Problem Measure The number of seasonal influenza-associated deaths varies from year to year because flu seasons are unpredictable and often fluctuate in length and severity. The CDC estimates that from the 1976-1977 season to the 2006-2007 flu season, flu-associated deaths ranged from a low of about 3,000 to a high of about 49,000 people (1). In 2013, the CDC published a model to quantify the annual number of influenza-associated illnesses and hospitalizations averted by influenza vaccination during the 2006–11 influenza seasons (2). Using that model the CDC estimated that vaccination resulted in 79,000 (17%) fewer hospitalizations during the 2012–13 influenza season than otherwise might have occurred. Especially in the primary care setting, providers are facing increasing difficulties to clarify "influenza-myths" as well as to identify burdens which keep patients from choosing or receiving the valuable vaccination. • Lack of a standard process to address preventive care, in general, leading to creation of unique solutions to this problem • Perceived inability to influence patient wishes and misinformation • Relative little involvement of clinic staff Goal Actual Lessons Learned Standard process Attd review • Doing an improvement project in isolation from the rest of the practice made it hard to create a standard way of checking vaccine status that would sustain itself • A standard process does not become the standard without effective training and reinforcement at first • Reliance on memory does not yield much improvement • We tended to make changes where we felt we had the most control, rather than trying to change patient beliefs, which was the greatest opportunity • Data collection should be built into the work flow or should come from a ready source What changes might result in an improvement? Aim Statement By January 1, 2014, 70% of more of all patients seen in the Friday resident clinic at 1525 Clifton Road will be vaccinated during their appointment (if not already completed). References Tests of Change (1) Thompson MG et al., Estimated Deaths Associated with Seasonal Influenza - United states 1976-2006, Weekly, August 27, 2010 / 59(33);1057-1062 (2) CDC. Prevention and control of seasonal influenza with vaccines. Recommendations of the Advisory Committee on Immunization Practices—United States, 2013–2014. MMWR 2013;62(No. RR-7). • Jan: Created standard process to let MD know patient’s status and wishes • Feb: Attending to review vaccine status during sign-out as detection and mitigation step.
Increasing Problem-Specific Educational Materials to Patients at the Emory Clinic Elizabeth Wiles DO, Paul F. La Porte MD PhD, Emory Hsu MD, Ross Deppe MD, Samantha Shams MD, Blake Anderson MD and Naveen Bellam MD MPH Faculty Mentor: David Propp MD The Emory Clinic at 1525 Clifton Rd, Emory University School of Medicine, Atlanta, GA Barriers Problem Statistical Measures and Analysis • Full schedules, clinic time constraints, or PCPs writing notes at the end of clinic did not benefit from computer-based educational templates. • There remains minimal incentive to create additional templates. • While desktop reminders were useful at first, physical notes could be lost , misplaced, or ignored. • Nurses had variability in providing reminders due to the multitude of patient tasks and multiple residents in clinic. • Patient illness complexity may not have had appropriate EMR-specific resource (i.e. providing education on PEG tube use, or proper explanation of more rare diseases). Physicians do not always effectively communicate medical problems or treatment plans to their patients and retention of education performed by the physician is an issue even among highly educated patients. Difficulty with understanding medical disease has been hypothesized to contribute to lower compliance with medication and activity regimens, increased calls to nursing staff, higher repeat visits, and worse medical outcomes. In 2012, the Center for Medicare/Medicaid Services (CMS) created the objective to use Electronic Health Records (EHR) to provide at least 10% of patients with electronically generated educational resources as part of their meaningful use criteria. Given a possible cost savings of $289 billion dollars from improved medication compliance alone, providing problem specific resources in a timely and appropriate fashion has potential to improve patient satisfaction and compliance in regards to their medical plans. Results Analysis Compared to CMS Objective as well as against Primary AIM Statement Baseline period (Prior to Test of Change): Rate = 8.0% Likelihood of 8.0% rate below CMS 10% rate?; p = 0.097 - It cannot conclusively be stated say that we were not already meeting “Meaningful Use” criteria 1st test of change: Handout rate 8.0% (before), 37.4% (after) % change over pretest period = 29.4% (22.6-36.2%) LR = 4.67 p < 0.0001 - 37.4% rate compared to CMS 10% goal; p << 0.0001 - During test of change 1, it cannot conclusively say we met our target of 30% absolute increase in handouts (CI is between 22.6-36.2) 2nd test of change: Handout rate 8.0% (before) vs 50.7% (after) % change over pretest period = 42.7% (30.6-54.7) LR = 6.32 p < 0.0001 - 50.7% rate compared to CMS 10% goal; p << 0.0001 - During test of change 2, we can conclusively say we met our target of 30% absolute increase in handouts (CI is between 30.6-54.7) 2nd test of change vs 1st test of change: Handout rate 37.4% (before) vs 50.7% (after) % change over 1st test of change period = 13.2 (-0.1-26.7) LR 1.35 (1.02-1.80) p = 0.0491 - Based on a p-value of less than 0.05, it can be stated there was a measurable difference between test of change 2 and 1 (i.e. MA reminders)… p = 0.0491 - The LR is significant compared to the p-value (double-checked with a different procedure) possibly due to separate calculations in software Baseline Study Data Data Chi-Squared Statistics Cause and Effect Analysis Tests of Change Test of change (TOC) 1: Educating physicians regarding use of standardized computer-based education format and use of a desktop reminder at each computer. Test of change 2: Require nurses reminders during their portion of the patient depart process if we had not chosen education for the patient using the above computer selected format. Lessons Learned A multifactorial and team-based approach can lead to improved patient awareness and education at a time cost not overly detrimental to clinic flow. Cost-effectiveness may be theorized to be appropriate and beneficial in improving patient outcomes; however, we do not have financial data to support this assertion. Importantly, focusing our intervention on an existing element not requiring any modification to the resident workflow was a key to success. MD Factors Forgetting to offer educational resources Nursing Factors Not remembering to provide / print education via depart process Checking out patients without nursing assistance Time constraints not allowing for nursing reminder Clicking on “Patient Education” opens all available educational resources based on diagnosis code, or per prompted search Aim Statement Acute visit time constraint Providing Patient Education Ease of Use Lack of insight Can not read To increase patient education handouts by 30% during the study period Nov 1 2013-Feb 14th 2014 (compared to July-October 2013), through entering education related to patient diagnoses in General Clinic note. Krames Database having appropriate education related diagnoses Patient feeling education Is unnecessary Implemenation Time and Time to Print Resources Patient factors System factors
PATIENT PHYSICIAN has not heard of 'code status' or AD I do not know how to initiate discussion Would like to discuss with family first Does not want to discuss Not enough time I forget Lack of continuity with patients Assigned patients are too young Not enough time in clinic visit Patients not prepared to discuss topic Inadequate reminder system SYSTEM Increasing End-of-Life Care Discussions, Including Code Status, in a Resident Run Urban Community Primary Care Clinic Orange Pod Wednesday/Friday Team, Grady Primary Care Center Rekha Thammana, MD, Andrew Ip, MD, Nurcan Ilksoy, MD, Shelly-Ann Fluker, MD, Dominique Cosco, MD Fofie Akota, MD, Stephen Berger, MD, Matthew Darrow, MD, Kendrick Gwynn, MD, Racha Halawi, MD, Elisa Ignatius, MD, Moise Jean, MD, Emma Johns, MD, Poonam Kalidas, MD, Christine Kirlew, MD, Enoch Kotei, MD, Song Li, MD, Jason Perry, MD, Nikita Patel, MD, Priyesh Patel, MD, Roshan Patel, MD, Deep Shah, MD, Sana Shah, MD, Yoo Shin, MD, Geoffrey Southmayd, MD, Komal D’Souza, MD, Xiao Jing Wang, MD, Andrew Webster, MD Barriers Problem Measure • Many elderly patients (defined as >65 years of age) do not have advanced directives on file • Discussing code status and end-of-life care is difficult given time constraints in our clinic visits • Residents have trouble initiating conversations about end-of-life care • Tests of change • Dot phrase added (TOC1) • To help providers remind about having code-status or advanced-directive discussions • Surveys passed in waiting room (TOC2) • Allows patients to ask provider questions about end-of-life-care • Not enough time! – patients often come in with a large agenda or have multiple chronic medical diseases • No standardized method to initiate code status discussions or end-of-life • Forgetting to implement dot phrase • No easy way to document code status in EPIC chart Lessons Learned What changes might result in an improvement? Aim Statement • Education of providers on palliative care discussions • Need for easier documentation methods in EPIC for advanced directives or code status • Education of patients to help facilitate discussions in outpatient visits • Physicians have little time to discuss, thus other methods must be implemented (nurse or group visits) • We aim to increase the number of end-of-life care discussions, including code status documentations, in Grady Orange Pod patients older than 65 years, to 50% by April 2014 Acknowledgement We would like to thank the nurses and support staff of the Orange Pod Primary Care clinic for their assistance with the project. End-of-Life care discussion has not been documented
Best Foot Forward Improving Performance and Documentation of Diabetic Foot Exams in an Urban Resident Primary Care Clinic Grady Primary Care Center, Wednesday Purple Pod James MacNamara, Matthew Dudgeon, Heather Batchelor, Annie Massart, Rahul Maheshwari, Jeffery Hedley, Maria Klimenko, Pooja Kotadia Faculty Mentor: Nurcan Ilksoy Problem Measure • Many diabetic patients present to the primary care clinic and go without consistent foot exams. • The American Diabetes Association recommends clinicians perform a comprehensive foot examination annually on patients with diabetes to identify risk factors for ulcers and amputation and perform a visual inspection of the feet at each visit.1 • Lavery, et al demonstrated a combined minor and major amputations reduction from 12.89 to 6.18 per 1000 patients per year with a diabetes foot prevention program.2 Others have shown significantly improved outcomes as well.3 First visit with pt, MD defers RHM til next visit Barriers • Not enough publicity of the foot exam techniques and guidelines • Inconsistent documentation amongst providers’ exams and assessments • Patient do not like having shoes off while waiting for provider • Patients unaware of need for foot exams • Limited Monofilaments, no tuning forks available in clinic What changes might result in an improvement? Aim Statement • Our aim was to increase the documentation of last complete diabetic foot exams and current inspection for known diabetic patients at Purple Pod Wednesday Primary care clinic visits by 50% by March 30th, 2014. Future Directions • A persisting method of encouraging exams is needed with involving nursing staff • A concise and complete dot phrase and may promote consistency amongst providers • Providing patients with information so they can advocate for the exam • Ensuring appropriate equipment is in every exam room • Boulton, et al Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care. 2008 Aug;31(8):1679-85 • Lavery La, Wunderlich RP, Tredwell JL. Disease management for the diabetic foot: effectiveness of a diabetic foot prevention program to reduce amputations and hospitalizations. Diabetes Res. Clin. Pract.2005; 70(1): 31–37. • Ozdemir, et al Population-based screening for the prevention of lower extremity complications in diabetes. Diabetes Metab Res Rev. 2013 Mar;29(3):173-82 First visit with pt, MD defers RHM til next visit