Download
1 / 67
670 likes | 766 Vues
When, how and which patient to treat with HBV infection. David Mutimer Queen Elizabeth Hospital Birmingham, England. BSG Post-graduate Course March 20 th 2006. WHO Global Burden of Disease 2000 Cirrhosis (all causes). 785,000 deaths per annum from liver failure (cirrhosis, all causes)

E N D
When, how and which patient to treat with HBV infection. David Mutimer Queen Elizabeth Hospital Birmingham, England. BSG Post-graduate Course March 20th 2006.
WHO Global Burden of Disease 2000Cirrhosis (all causes) • 785,000 deaths per annum from liver failure (cirrhosis, all causes) • HBV 40% • HCV 25% • Other causes 35% • 600,000 deaths per annum from HCC • HBV 57% • HCV18% • Other causes 25%
WHO Global Burden of Disease 2000Mortality from HBV & HCV • 1 million deaths per annum • including deaths from cirrhosis and/or liver cancer • HBV causes 644,000 deaths per annum • HCV causes 325,000 deaths per annum
= who? When , how and which patient to treat with HBV infection. David Mutimer Queen Elizabeth Hospital Birmingham, England. BSG Post-graduate Course March 20th 2006.
Where do carriers come from?
Where do carriers come from? Acute infection <5% risk Chronic infection “carrier”
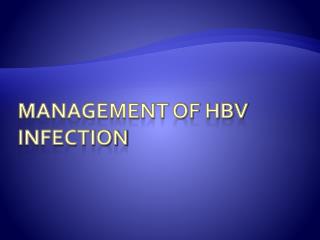
Transmission of HBV in England & WalesHahné et al J Clin Virol 2004;29:211-220. Acute HBV infection n=2,876 Resolution & immunity n=2,660 Chronic infection n=216
Transmission of HBV in England & WalesHahné et al J Clin Virol 2004;29:211-220.
Transmission of HBV in England & WalesHahné et al J Clin Virol 2004;29:211-220. New chronic infections in England & Wales (per annum) • Arising in E & W • n = 216 (3%) • Coming from abroad • n = 6,571 (97%)
Where do carriers come from? “carrier” from abroad Acute infection <5% risk Chronic infection “carrier”
Where do carriers come from? “carrier” from abroad Acute infection <5% risk Chronic infection “carrier”
HIGH-LEVEL REPLICATION HBeAg+ve LOW-LEVEL REPLICATION 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve LOW-LEVEL REPLICATION 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve LOW-LEVEL REPLICATION 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve LOW-LEVEL REPLICATION 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve LOW-LEVEL REPLICATION 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBV DEATH HBeAg-ve LOW-LEVEL REPLICATION 40 50 0 20
Liver Transplantation for Chronic HBVUK Transplant data : 1990-2003 Male:female 297:47 (6:1) Median age 50
= who? When , how and which patient to treat with HBV infection. David Mutimer Queen Elizabeth Hospital Birmingham, England. BSG Post-graduate Course March 20th 2006.
When , how and which patient to treat with HBV infection. David Mutimer Queen Elizabeth Hospital Birmingham, England. BSG Post-graduate Course March 20th 2006.
HIGH-LEVEL REPLICATION HBeAg+ve • Aim of Treatment • HBeAg seroconversion • Choice of treatment • Interferon • Lamivudine • Adefovir • But! • High rate of spontaneous seroconversion • Little increase with treatment • A lot of females! 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve • Aim of Treatment • HBeAg seroconversion • Choice of treatment • Interferon • Lamivudine • Adefovir • But! • High rate of spontaneous seroconversion • Little increase with treatment • A lot of females! 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve • Aim of Treatment • HBeAg seroconversion • Choice of treatment • Interferon • Lamivudine • Adefovir • But! • High rate of spontaneous seroconversion • Little increase with treatment • A lot of females! 40 50 0 20
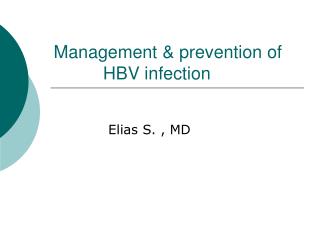
Spontaneous HBeAg SeroconversionItalian children Bortolotti et al J Hep 1998 168 HBeAg +ve Median age 5 at entry
Spontaneous HBeAg SeroconversionItalian children Bortolotti et al J Hep 1998 168 HBeAg +ve Median age 5 at entry HBeAg seroconversion @ 8% per annum
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy – I wouldn’t
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy – I wouldn’t • ? antiviral treatment
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy – I wouldn’t • ? antiviral treatment – I wouldn’t
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy – I wouldn’t • ? antiviral treatment – I wouldn’t • what happened next?
Case 1 • 20 year old Asian lady • HBeAg-positive • ALT 50, other LFT’s normal • ? liver biopsy – I wouldn’t • ? antiviral treatment – I wouldn’t • what happened next? • annual review • spontaneous HBeAg seroconversion 2 years later
HIGH-LEVEL REPLICATION HBeAg+ve • Replication after 40 • Death wish • Always treat! • Aim of treatment • HBV suppression • (HBeAg seroconversion) • Choice of treatment • Lamivudine • Adefovir • (Interferon) HBV DEATH HBeAg-ve 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve • Replication after 40 • Death wish • Always treat! • Aim of treatment • HBV suppression • (HBeAg seroconversion) • Choice of treatment • Lamivudine • Adefovir • (Interferon) HBV DEATH HBeAg-ve 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve • Replication after 40 • Death wish • Always treat! • Aim of treatment • HBV suppression • (HBeAg seroconversion) • Choice of treatment • Lamivudine • Adefovir • (Interferon) HBV DEATH HBeAg-ve 40 50 0 20
Case 2 • 47 year old Chinese male • HBeAg-negative • ALT 55 • what else?
Case 2 • 47 year old Chinese male • HBeAg-negative • ALT 55 • what else? • HBV DNA 500,000 copies/ml • US heterogeneous liver • liver biopsy
Case 2 • 47 year old Chinese male • HBeAg-negative • ALT 55 • what else? • HBV DNA 500,000 copies/ml • US heterogeneous liver • liver biopsy • antiviral treatment?
Case 2 • 47 year old Chinese male • HBeAg-negative • ALT 55 • what else? • HBV DNA 500,000 copies/ml • US heterogeneous liver • liver biopsy • antiviral treatment? • definitely – with nucleosides
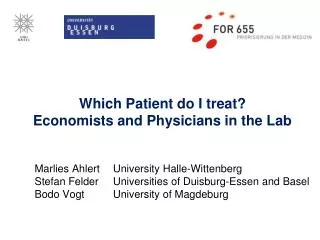
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve • Observe? • Further spontaneous selection likely • Females > males • 20’s > 30’s • Reduces costs (indefinite duration of • treatment) • Reduces toxicity (cumulative) • Family planning • Fibrosis is reversible! • Treat? • High risk population • Lowest risk have “self-sorted” • Males > females • 30’s > 20’s • Suppression prevents fibrosis • Indefinite suppression possible! 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve • Observe? • Further spontaneous selection likely • Females > males • 20’s > 30’s • Reduces costs (indefinite duration of • treatment) • Reduces toxicity (cumulative) • Family planning • Fibrosis is reversible! • Treat? • High risk population • Lowest risk have “self-sorted” • Males > females • 30’s > 20’s • Suppression prevents fibrosis • Indefinite suppression possible! 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve • Observe? • Further spontaneous selection likely • Females > males • 20’s > 30’s • Reduces costs (indefinite duration of • treatment) • Reduces toxicity (cumulative) • Family planning • Fibrosis is reversible! • Treat? • High risk population • Lowest risk have “self-sorted” • Males > females • 30’s > 20’s • Suppression prevents fibrosis • Indefinite suppression possible! 40 50 0 20
HIGH-LEVEL REPLICATION HBeAg+ve HBeAg-ve • Observe? • Further spontaneous selection likely • Females > males • 20’s > 30’s • Fibrosis is reversible? • Reduces costs (indefinite duration of • treatment) • Reduces toxicity (cumulative) • Family planning • Treat? • High risk population • Lowest risk have “self-sorted” • Males > females • 30’s > 20’s • Suppression prevents fibrosis • Indefinite suppression possible? 40 50 0 20