Download
1 / 51
520 likes | 632 Vues
Т ASHKENT MEDICAL ACADEMY. Department of Infectious and pediatric infectious diseases Lecturer: Doc . Yakubov.X.K . Theme: Early and Comparative diagnosis of deseases with the syndrome of meningitis and meningoencephalitis . Tashkent -20 11. Р lan :. Introduction – 5 min .

E N D
ТASHKENT MEDICAL ACADEMY Department of Infectious and pediatric infectious diseases Lecturer:Doc.Yakubov.X.K. Theme:Early and Comparative diagnosis of deseases with the syndrome of meningitis and meningoencephalitis. Tashkent-2011
Рlan: • Introduction – 5 min. • Etiology, epidemiology and order of the theme- 15min. • Differential diagnosis of deseases which have mostly met with the syndrome of meningitis and meningoencephalitis- 60min.. • Conclusion- 10 min. • Total: 90 min- 2 academic hours
Меningeal syndromes (MS)- is the complex signs of the brain meninges are being irritated. Encephalitic syndrome -is the complex signs of the brain substance is being irritated.
Meningeal syndromes are divided into 2 groups:1. General brain symptoms.2. Special meningeal symptoms.
1.General brain symptoms: - severe headache with the straining terrible character - vomiting, not bringing the patient to facilitate - psychomotor agitation - delusions,hallucinations,convulsions - varicose veins in the fundus - children monotonous “brainscream” - coma ,sopor
2. Special meningeal symptoms: - hyperesthesia ( for light and sound ) - tonic muscle tension 1) stiff neck 2) Kernig’s symptom,the symptoms Brudzinsk 3) symptom “Lesage or suspension in infants 4) bulging of the large fontanel in infants
- reactive pain phenomenas: 1) pain with the pressure on the eyeballs 2) pain on the front wall of the external meatus 3) increasing headache for percussion zygomatic arches and the skull - reduction in abdominal,periosteal and tendon reflexes
II.Pseudomeningitis-characterized by clinical manifestations and cerebral meningeal symptoms without inflammatory changes in SF.
Classification of meningitis and meningoencephalitis I. А. PrimaryB. Secondary II.According to etiology 1 bacterial 3 rickettsial 5 viral 7 protozoal 2 fungal 4 helminth 6 spirochetal 8 mixed III.By the nature of the CSF 1- purulent 2- serous IV.According to the degree of gravity 1- light 2- middle 3- heavy V. Кечиши буйича А By the character:1. smooth 2. not smooth а) with complications b) with secondary infection c) with the aggravation of chronic diseases Б. According to duration: 1. Acute 2. Prolonged 3. chronic
Purulent meningitis snd meningoencephalitis Meningitis and meningoencephalitis arisen as an independent disease. Meningitis and meningoencephalitis caused by eningococcal,pneumococcal and stick Pfeiffer.
Meningococcal meningitis and M.E Acute human infection desease is caused by meningococ Transmitted by airborne droplets More met in children and young persons Seasonality of the winter-spring Main way of the sreading the activator in the body is hematogenically 50% of patients precede the symptoms of nasopharyngitis(1-5 days)
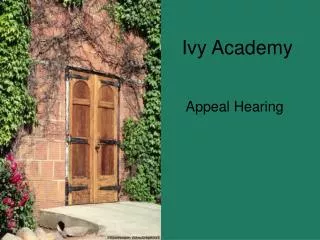
Positive Kering’s symptom - Bending the legs in the hip joint is impossible to straighten the knee
Meningococcal meningitis • The desease begins with fever, temperature rises to 39-40 ˚,severe headache,vomiting, hyperesthesia,pain in the eyeball • Repeated vomiting does not bring relief • In 2-3 days meningeal symptoms appear : stiff neck, sympoms Kering and Grudzinsk • hyperesthesia • The appearance of symptoms of local points to edema-swelling of the brain. • Reduction of abdominal and tendon reflexes • Hyperskeocytosis- in the blood of the patient, stab shift, eosinophilia, ESR increased up to 45-70mm/h.
Meningococcal meningitis In young children can join convulsions, meningeal symptoms are mild,but there are a symptom Lessagebulging of the large prefontanel,hand tremor,crowding of the head and the end of the first day the patient takes characteristic pose “setter dog”
Meningococcal meningoencephalitis Encephalitik symptoms: stimulation in acting, violation of consciousness,convulsions,lesion of III, IV, V, VIII, less often than other cranial nerves Hemi- and monopharesis Bulbar paralysis,cerebellar ataxy, disorders in oculoactions
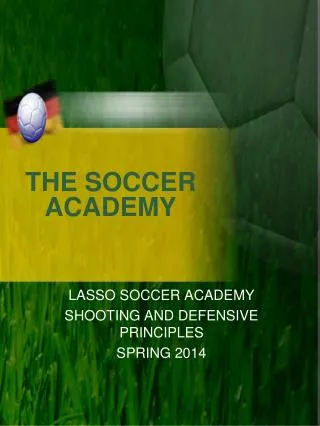
1.The patient’s position during lumbar puncture.2.The liquid of the back brain.3. “Festering cap”in meningococcal meningitis.
The main likvorological signs in meningitis Signs Normal likvor Serous meningitis Purulent meningitis Color and clarity Colorless, clear Colorless, clear Whitish or green, muddy Pressure(in mm of water .up.) 130-180 200-250 increased The speed of leakage from the needle 40-60 60-90 Jet Cytosis(number of cells in 1mm) 2-8 20-800 1000-1500 and more Cytogram: Limphocytes % Neutrophils% 80-85 3-5 80-100 0-20 0-60 40-100 Protein 0,25- 0, 33 0,33-1,0 0,66- 16,0 Reaction”Pandi” «neg» + (++) +++( ++++)
Pnemococcal meningitis and meningoencephalitis - occur as sporadic disease - 20-30 % consists of all purulent meningitis - more common in young children - contribute to the development of old injured skull -most often affects the brain tissue (80%) - none bacteremia (hemorr.rash) - early and more frequent loss of consciousness,spasm
Primary ameobic meningoencephalitis(amp) Observed very rarely Suddenly develops In the beginning the signs of pharyngitis are found Then severe haedaches,vomiting,a very high temperature Rapidly groving disturbance of consciousness(sopor,coma) Signs of acute purulent meningitis combined with focal symptoms (encephalitis)
Meningitis of Pfeyffer Activator is bacillus Pfeiffer The activator is found in the mucosa of the upper respiratory tract in helthy people Can cause pneumonia, meningitis ,etc. More common in children under 2to 3 years
There is an acute form of purulent meningitis Develops septicemia The temparature of the body is very high The phenomena of conjunctivis, bronchitis,pneumonia The appointed pencillin does not give effect The clinic of Pfeyffer meningitis in young adults
Prevention of meningococcal infection • Discharge of patients after complete recovery • For the active immunization vaccines used: -vaccine A (Russia) -vaccine V (VamegosBS, Cuba) -divalent “MeningoA+C” (France) Early isolation of sick or bacillicariers. Quarantine in a collective where the patient indentified,for a period 10 days daily inspection of skin and thermometry For contacted- anlysis from the nasopharynx at least 2 times with an interval 3-7 days. For contacted- immunoglobulin at dose 1.5-3.0ml for prevention
Serous meningitis and meningoencephalitis According to etiology: viral, bakterial According to development: primary,secondary
Primary serous meningitis and meningoencephalitis 1. limphocytic horeomeningitis 2. meningitis toxoplasmosis 3. ticky meningitis 4. japan encephalitis 5. tuberculous meningitis
Acute lymphocytic horiomeningitis (A.L.H) - is 2-5 % of all serous meningitis - in 60% of patients the desease begins as an isolated meningitis or meningoencephalitis - with the beginig 30% of patients have high temperature(4-6days), intoxication - development after a catarrhal inflamation of muscous membranes is 10% - after some time the signs of meningitis begin to appear
Toxoplasmosis meningoencephalitis - - develops in individuals with chronic or latent infection - generalization is met with the weakening of immunity(radiation therapy,the use of immunosuppressive drugs, hormones and in AIDS) - the temparature of the patient is 39-40 degrees,severe headache - vomiting,hallucinations, convulsions - violation of the cranial nerves - paresis and paralysis of limbs - myositis, liver enlargement, calcification in the brain
Otogenic Septic Streptococcal Esherihiozik Etc Secondary purulent meningitis and meningoencephalitis are distinguished:
In otogenic meningitis bacterials penetrate the meninges by • By contact • By vascular way Distinguishes: Labirintogenic meningitis Timpanogenic meningitis
The clinic of otogenic meningitis • Meningitis develops rapidly • There sudden severe headache • Temperature is 39-40 degrees, persistent vomiting • The patient quickly loses consciousness • Meningeal symptoms are quickly found • In the first hours of the development of meningitis the congested optic disks can be seen • The outcome is serious , possibly death after 24-48 hours
In the otogenic purulent meningitis affects • For the first the membranes of the base brain • Then tne posterior fossa • Rigidity of the muscles of the back of the head • Early and sudden expressed than symptoms Kernig and Brudzinsk
Likvorologikal changes in otogenic meningitis • SF is turbid • Cytosis is neutrophil • Protein is increased
Tuberculous meningitis Starts gradually, 7-14 days subferbilitet Weakness, fatigue Drowsiness, then insomnia Loss of appetite, constipation, vomiting Autonomic vascular disorders(red spots on the body, spots of Trusseau )
The clinic of the tuberculous meningitis at the height of the desease • Bradycardia followed by tachycardia • Headache grows to 2-3 weeks • Very sudden • Temperature is 38-39 • MS is gradually increased
Secondary serous meningitis and meningoencephalitis Parotitic Measless Influenzal
Parotitic meningitis Etiology: The causative agent of parotid infection is an RNA-containing virus Pneumophilis parotidis, which belongs to the paramyxovirus with dimensions of 35 nm to 540nm Antigens of parotid virus: 1.Antigen V associated with the virion(infectious) 2. Antigen S, slouble, in smaller sizes (noninfectious)
Epidemiologic parotit:the increase of parotid gland in the right
The diagnosis: • Epidanamnez • Objective facts. 3. Lymphocitosis • Amylase in the blood or urine • Analysis with diabetic feature. • SF research. • Serological research,Intradermal reaction.
Acute lymphocytic horiomenigitis • 2%-5% of serous meningitis • In 60% of patients the disease begins as an isolated meningitis or ME • In 30% the appearance preceded with high temperature(4-6 days), intoxication • 10% of patients develops after a catarrhal inflammation of mucous membranes
The clinic acute lymphocytic horiomenigitis • The initial fever lasts 2-3 days • After that short-term remission • The temperature is 39 degrees again and above • Chills, severe headache, vomiting • Pain in the eyeballs, myalgia • A few hours later rigidity, Kernig and Brudzinskogo symptoms • Sometimes symptoms of encephalitis