Download
1 / 48
480 likes | 953 Vues
Influenza Vaccination Seminar “ Learn the Facts N ’ Get a Shot TODAY! ” Oct 2007 Prepared by Infection Control Branch, CHP Infectious Disease Control Training Centre, HAHO Content outline Influenza situation in Hong Kong Situation update on H5 Influenza

E N D
Influenza Vaccination Seminar“Learn the Facts N’ Get a Shot TODAY!”Oct 2007 Prepared by Infection Control Branch, CHP Infectious Disease Control Training Centre, HAHO
Content outline • Influenza situation in Hong Kong • Situation update on H5 Influenza • Influenza vaccination suggestions by CHP • HA influenza Vaccination program 2007/08
Important messages • H3N2 remains to be the predominant strain over the past 3 years • No H5, H7, or H9 human case in Hong Kong last year
Breakdown of confirmed human cases of avian influenza A (H5N1) as of 10 Sept 2007 ( 12 countries)
Summaryof current situation of H5 influenza • Endemic in South East Asia • Increasing in geographical area • Increasing in affected host range • Limited human-to-human transmission has occurred (family cluster in Thailand September 2004 and in Indonesia May 06) • Atypical clinical presentation For details pls refer to Risk Assesssment of Influenza A H5N1 Pandemic version 10Sep07 http://ha.home/idctc/document/risk_assessment_of_ai__predispositions_influenza_pandeminc_10_sep_07.pdf
Risk AssessmentClinical Features • Risk of fecal-oral transmission? • Case fatality rate (CFR) around 60% • Incubation period: 2-10 days; 3-7 days • Atypical presentations: diarrhea & encephalitis • Asymptomatic or Mildly symptomatic infections Summary of Case-fatality rate (CFR) of the human cases of avian influenza A (H5N1) by onset of year and age group (WHO weekly epidemiological record No 26,2006,81, 249-260)
WHO recommendation for influenza vaccine for the year 2007/2008 • Northern hemisphere • An A/Soloman Islands/3/2006(H1N1)-like virus • An A/Wisconsin/67/2005(H3N2)-like virus • A B/Malaysia/2506/2004-like virus
Rationale • Most people are ill with flu for a few days • Some may get more severe signs and symptoms or be even fatal, especially for elderly & immunocompromized • Flu vaccine is documented to reduce infection and complication rates • Vaccination will not protect humans from H5N1 infection, but it minimizes the risk of co-infection and genetic reassortment of human and avian influenza viruses in humans
Scientific Committee on Vaccine Preventable DiseasesStatements on Influenza Vaccination for the 2007/08 Season • Elderly Persons Living in Residential Care Homes • Long-stay Residents of Institutions for the Disabled • Elderly Persons Aged 65 Years or Above • Persons with Chronic Illnesses • Health Care Workers • Poultry Workers • Children aged 6 to 23 months • Pregnant women
Targeted Groups of HA program • In-patient (IP) of infirmary, psycho-geriatric, mentally ill and mentally handicapped units/wards, and hospitalized patients with chronic diseases under HA • Paediatric IP & Out-patient (OP) with chronic diseases, or on long term aspirin therapy • Non-institutionalized elderly aged 65 or above with chronic illness and followed up in public clinics • Poultry workers and those who may be involved in poultry culling operations • Comprehensive Social Security Assistance (CSSA) recipients under the following categories*: a) Persons with chronic diseases regardless of age b)Elderly aged 65 or above* c) Children aged 6-23 months from families receiving CSSA* d) All pregnant women with antenatal FU in public clinics
Why Healthcare workers need to be vaccinated? • To REDUCE the risk of transmitting influenza to patients who are at high risk of complications from influenza • To REDUCE absenteeism among health care workers related to respiratory infections • Influenza vaccination is recommended for ALL health care workers
Targeted HCW • HA staff (including part time, contract and temporary staff) • Civil servants under HA management or whose normal place of work is in HA hospitals or clinic compounds (e.g., E&M staff) • Contract out colleagues who have direct patient care or work in a patient-care environment • Registered hospital volunteers
HCW for RCHE and RCHD • There is strong local and overseas evidence that influenza vaccination is effective in reducing the risk of complications from influenza among elderly persons living in residential care homes. • Local data shows that long-stay residents of institutions for the mentally and physically disabled have high rates of hospitalization during influenza outbreaks
Timing on flu vaccine • Vaccine composition is updated every year • Protection develops about 2 weeks after vaccination • The best time for vaccination is October to December
Precautions • Consult the doctor or nurse in charge of staff vaccination program in your hospital before getting a flu shot if you have • Serious egg allergic reactions or reactions to previous influenza vaccine; allergy to neomycin • History of severe paralytic disease called Guillain-Barre Syndrome (GBS) • Moderate to severe acute illness
Side effects (Mild) - No need to report • Soreness, redness, or swelling where the shot was given • Fever • Aches If these problems occur, they usually begin soon after the shot and last 1-2 days
Side effects (severe) • Severe side effects associated with influenza vaccine are very rare • They include severe allergic reactions, severe local reactions, & neurological complications
Side effects (severe) Within 24 hours of immunization • Anaphylactoid reaction • Anaphylaxis • Severe allergic reaction (e.g. angioedema and allergic asthma) Within 5 days of immunization • Severe local reaction • Sepsis • Injection site abscess (bacterial / sterile)
Side effects (severe) Within 15 days of immunization • Seizure & Encephalopathy Within 3 months of immunization • Neurological disorders, such as Guillain-Barre Syndrome, encephalomyelitis, neuritis • Vasculitis • Neuralgia & Paraesthesia • Thrombocytopenia
Guillain-Barre Syndrome (GBS) and flu vaccine • In 1976, swine influenza vaccine was associated with GBS. Since then, flu vaccines have not been clearly linked to GBS. • However, if there is a risk of GBS from current flu vaccines, it would be no more than 1 or 2 cases per million people vaccinated. • It peaks 2 weeks after vaccination and usually within 3 months of the vaccination. • This is much lower than the risk of severe influenza, which can be prevented by vaccination Lasky T et al. NEJM 1998; 339: 1797- 1802
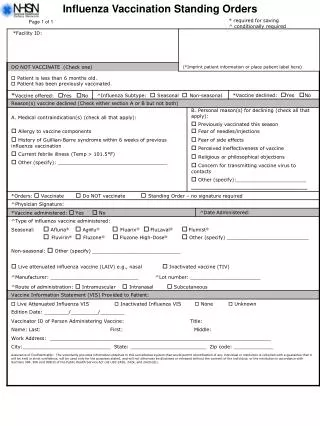
Adverse Reaction Report Form ONLY severe adverse reactions are required to be reported Note: Also report any death, hospitalization or other severe & unusual events thought to be related to immunization
Information Package on ha.home • Information kit prepared for patients & staff • SOPD / GOPD • Staff • Time schedule • Information pamphlet • Vaccination adverse reaction reporting form • Weekly return form from GOPD/SOPD HA Influenza Vaccination Program 2007/08
Logistics • Referral not required • Staff consent form • For all patients (in-patients & out-patients), a consent from patient suffices • Adult immunization card for both public and private sector with effect from Oct 2007
Logistics - Staff • HCEs are required to make arrangement / derive plan to vaccinate their staff • Alternatively, hospital colleagues may make arrangement for vaccination via the normal booking system at any of the 8 designated staff clinics • HAHO staff may make arrangement for vaccination through the 8 designated staff clinics • DH will make separate arrangement for poultry-related workers.
Patient Consent Form • Staff Consent Form
HA Influenza Vaccination Programme 2007/08Time Schedule of Vaccination
Knowledge Gap of HCWs and the Truth of Flu vaccine • Misconception of flu vaccine: • Belief that they’re not at risk • Ignorance regarding the risk they represent to their patients • Inappropriate knowledge about vaccine efficacy • Fear of needles • Ignorance about the vaccine (eg it causes the flu)
Misconceptions : the consequences • Fears emotionally driven and not based on data • As a result, HCWs don’t get the vaccine, nor do their patients • “ We have met the enemy and he is us”
Influenza Vaccine Efficacy • Defining efficacy is important • The vaccine’s benefit is in preventing hospitalization and death, not symptoms • The vaccine • - reduce death: 50-85% • - reduces illness : 30-70% • - reduces lower respiratory tract involvement:70-90%
Knowledge Gap of HCWs and the Truth of Flu vaccine • Facts: • Epidemiology of seasonal flu is clear • Flu vaccine efficacy is clear • S/E of flu vaccine is clear • BENEFITS >>> HARMS for flu vaccine is clear
Knowledge Gap of HCWs and the Truth of Flu vaccine • Belief: Do you believe in the figures? • Burden: Do you think HK has a similar flu morbidities and mortalities? • Budget: Does it cost anything to get a shot? • Barrier: Any barrier from admin/logistics/people/workflow? • Biology: Is your body build different from the people being investigated?
“Learn the Facts N’ Get a Shot TODAY!” • “Learn the Facts N’ Get a Shot TODAY!” • Benefits: Save lives, prevent health care disruptions, prevent hospitalizations • Benefits HCWs • Patient safety issue- benefits the patient (esp. immunocompromised hosts increasing) • Benefit hospitals and clinics • Set a good example for our patients • Be smart and ASK questions to your doctor-in-charge.
Intervention known to increase immunization rates • The rates can be increased using methods demonstrated to work • eg. strong recommendation from a trusted health care provider • Immunization requirement
Acknowledgements • CCID-ER • CICO • SEB, CHP • PHLC • Dr Dominic Tsang, QEH
THANK YOU “Learn the Facts N’ Get a Shot TODAY!”