Download
1 / 28
280 likes | 682 Vues
Article:. Chang, K.W.

E N D
1. Practical Grading System for Evaluating Cisplatin Ototoxicity in Children K30 Journal Article Review
Denise Nicholson, Au.D., Ph.D. candidate
Senior Audiologist
Dept of Audiology I wanted to present an article, related to my field, that would have clinical applications to some of you here today. I wanted to present an article, related to my field, that would have clinical applications to some of you here today.
2. Article: Chang, K.W. & Chinosornvatana, N. (2010). Practical Grading System for Evaluating Cisplatin Ototoxicity in Children. Journal of Clinical Oncology, 28 (10), 1788-1795. This article was published in the Journal of Clinical Oncology just a few months ago. This article was published in the Journal of Clinical Oncology just a few months ago.
3. Background
Article
Clinical applications/future research The order of the presentation will be as follows. First, I will give you all a brief background and audiology tutorial. Next, I will present the details and findings within the article. Lastly, I will discuss clinical applications and areas of possible future research.The order of the presentation will be as follows. First, I will give you all a brief background and audiology tutorial. Next, I will present the details and findings within the article. Lastly, I will discuss clinical applications and areas of possible future research.
4. Background Cisplatin is used in the treatment of several childhood malignancies.
Improvement in long-term survival has made the monitoring of long-term side effects more important.
Nephrotoxicity and high frequency hearing loss are the most notable adverse effects of cisplatin in children
5. Audiometry Types of hearing loss
Conductive (CHL)- a hearing loss resulting from something affecting the outer or middle ear.
Possible causes include:
Cerumen impaction
Serous otitis media
Tumor
Sensorineural (SNHL)- A permanent type of hearing loss that may be congenital, due to inner ear or auditory nerve damage, and may be the result of noise exposure, genetics, or ototoxic medications.
May affect certain frequencies more than others
May cause distorted sound quality
Severity can range from mild to profound
May be late onset, stable, or progressive in nature
Mixed � Combination of CHL and SNHL There are 3 types of hearing loss. Today, we will focus on sensorineural hearing loss resulting from exposure to ototoxic medications, specifically, cisplatin and carboplatin.There are 3 types of hearing loss. Today, we will focus on sensorineural hearing loss resulting from exposure to ototoxic medications, specifically, cisplatin and carboplatin.
6. Implications of HFHL in Children Unable to hear certain speech sounds
Distortion
Speech understanding in noise
phonics (reading)
The implications of HFHL in children are often much more debilitating in children than adults. If you look to the right on the screen, there is a graph called an audiogram. An audiogram is used to plot the softest levels a person is able to hear pure-tones. The yellow shaded region on the graph is called a speech banana. It represents the range on the graph where speech sounds occur. If you look, a person must have access to very soft high frequency sounds in order to hear s, t, sh, th, and f sounds. These are the distinguishing characteristics of speech. Hearing loss due to ototoxic medications effects the basal end of the cochlea (hearing organ) first. So, the highest frequencies are initially affected, and subsequently lower frequencies may also be affected. With hearing loss of even a �mild� degree, a child often experiences marked difficulties compared to normal hearing peers. Understanding classroom instruction, especially if a teacher turns away from the student (to write on the board) or in the presence of competing noise poses various problems for children with even mild high frequency hearing loss. The implications of HFHL in children are often much more debilitating in children than adults. If you look to the right on the screen, there is a graph called an audiogram. An audiogram is used to plot the softest levels a person is able to hear pure-tones. The yellow shaded region on the graph is called a speech banana. It represents the range on the graph where speech sounds occur. If you look, a person must have access to very soft high frequency sounds in order to hear s, t, sh, th, and f sounds. These are the distinguishing characteristics of speech. Hearing loss due to ototoxic medications effects the basal end of the cochlea (hearing organ) first. So, the highest frequencies are initially affected, and subsequently lower frequencies may also be affected. With hearing loss of even a �mild� degree, a child often experiences marked difficulties compared to normal hearing peers. Understanding classroom instruction, especially if a teacher turns away from the student (to write on the board) or in the presence of competing noise poses various problems for children with even mild high frequency hearing loss.
7. Normal Hearing and Degrees of HL There is a continuum of the different degrees of hearing. Some frequencies may require more volume for a person to hear than another frequency. This is called the configuration of hearing loss. The term �mild hearing loss� may be misrepresentative. The term �mild� implies little difficulty, but the truth is, even a mild hearing loss may have serious educational implications and may require use of amplification or other types of assistive devices or strategies to ensure the child has proper access to auditory information in the classroom. Providing preferential seating to children with hearing loss may significantly help a child with this type/degree of hearing loss.
There is a continuum of the different degrees of hearing. Some frequencies may require more volume for a person to hear than another frequency. This is called the configuration of hearing loss. The term �mild hearing loss� may be misrepresentative. The term �mild� implies little difficulty, but the truth is, even a mild hearing loss may have serious educational implications and may require use of amplification or other types of assistive devices or strategies to ensure the child has proper access to auditory information in the classroom. Providing preferential seating to children with hearing loss may significantly help a child with this type/degree of hearing loss.
8. Difficulties Testing Children Age dependent test procedures
Bedside audiograms
Background noise
Not up to the task
Limited attention span
Sedated ABRs & other objective measures can be utilized
Testing hearing in children can be difficult for an audiologist. The test procedures used are age and development dependent. 1 � - 2 � year olds are the most difficult children to test behaviorally. When you add bedside testing to the equation, the difficulties increase dramatically. There is often competing background noise and the child just may not be up to testing. It is difficult to listen attentively to very soft tones, especially when you�re not feeling well. So, what are some other objective options? Well, there is an auditory brainstem response test, which must be utilized under sedation, but it gives us a very reliable picture regarding the child�s hearing. Testing hearing in children can be difficult for an audiologist. The test procedures used are age and development dependent. 1 � - 2 � year olds are the most difficult children to test behaviorally. When you add bedside testing to the equation, the difficulties increase dramatically. There is often competing background noise and the child just may not be up to testing. It is difficult to listen attentively to very soft tones, especially when you�re not feeling well. So, what are some other objective options? Well, there is an auditory brainstem response test, which must be utilized under sedation, but it gives us a very reliable picture regarding the child�s hearing.
9. Chang & Chinosornvatana (2010) Purpose:
Present a new ototoxicity grading system, with clearly defined audiometric criteria.
Validation of the grading system
Correspondence to audiology treatment recommendations
Compared with currently utilized Common Terminology Criteria for Adverse Events (CTCAE) Chang and his colleague decided to develop a modified version of the Brock ototoxicity grading scale and to compare that newly developed scale with the original brock scale and with the CTCAE scale. Their goal was to clearly define audiometric criteria as well as validate the modified grading system by establishing correspondence between the given grade and audiology treatment recommendations. Chang and his colleague decided to develop a modified version of the Brock ototoxicity grading scale and to compare that newly developed scale with the original brock scale and with the CTCAE scale. Their goal was to clearly define audiometric criteria as well as validate the modified grading system by establishing correspondence between the given grade and audiology treatment recommendations.
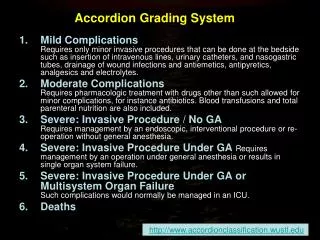
10. CTCAE Pediatric Grading Scale Based on 1,2,3,4,6, & 8 kHz
Grade 1
Threshold shift >20dB at 8kHZ in at least 1 ear
Grade 2
Threshold shift >20dB at 4kHz and above in at least 1 ear
Grade 3
HL sufficient to indicate therapeutic intervention including hearing aids
Threshold shift >20dB at 3kHz and above in at least 1 ear
Speech and language svcs indicated
Grade 4
Audiologic indication of cochlear implant
Speech and language svcs indicated The CTCAE grading scale assigns a numerical value grade, ranging from 1-4 based on the severity of the threshold shift affecting high frequencies. A threshold shift compares the baseline thresholds to current thresholds. A threshold shift greater than 20dB at 8kHz only is assigned at 1. If the child experiences a threshold shift > 20dB at 4kHz or above, in at least one ear, the child is assigned a grade of 2, and so on. With grade 3 and 4, the scale includes use a subjective criteria in addition to a frequency specific degree threshold shift. So, whether or not a child it is recommended for the child to receive speech and language services. The CTCAE grading scale assigns a numerical value grade, ranging from 1-4 based on the severity of the threshold shift affecting high frequencies. A threshold shift compares the baseline thresholds to current thresholds. A threshold shift greater than 20dB at 8kHz only is assigned at 1. If the child experiences a threshold shift > 20dB at 4kHz or above, in at least one ear, the child is assigned a grade of 2, and so on. With grade 3 and 4, the scale includes use a subjective criteria in addition to a frequency specific degree threshold shift. So, whether or not a child it is recommended for the child to receive speech and language services.
11. Brock Pediatric Grading Scale The brock grading scale assigns a numerical grade based on degree of bilateral hearing loss, but the inclusion criteria is less conservative. Also, the brock scale does not look at a threshold shift, rather the scale assesses the overall bilateral hearing loss. So, a bilateral hearing loss less than 40dB is given a grade of zero. In audiology, if a child came into my office with a flat 35dB sensorineural hearing loss, or even 35dB SNHL at 2-6kHz, I would recommend hearing aids. Like I mentioned previously, the term �mild� hearing loss can be misleading because it implies that functionally, this person should have minimal difficulties. With children, educational implications of even mild hearing loss can be substantial. The brock grading scale assigns a numerical grade based on degree of bilateral hearing loss, but the inclusion criteria is less conservative. Also, the brock scale does not look at a threshold shift, rather the scale assesses the overall bilateral hearing loss. So, a bilateral hearing loss less than 40dB is given a grade of zero. In audiology, if a child came into my office with a flat 35dB sensorineural hearing loss, or even 35dB SNHL at 2-6kHz, I would recommend hearing aids. Like I mentioned previously, the term �mild� hearing loss can be misleading because it implies that functionally, this person should have minimal difficulties. With children, educational implications of even mild hearing loss can be substantial.
12. Patients 134 pediatric patients
Received cisplatin or carboplatin
Audiologic evaluation performed during 105 (70.5%) of 149 treatment courses
90 had audiograms measured after @ least one dose of cisplatin or carboplatin
81 received cisplatin, of which, 67 received cisplatin as their only primary ototoxic chemotherapeutic agent
14 � cisplatin & carboplatin
9 � carboplatin only
In the Chang study, there wee 134 pediatric patients total receiving either cisplatin or carboplatin. In the Chang study, there wee 134 pediatric patients total receiving either cisplatin or carboplatin.
13. Methods Retrospective chart review
Audiologic
Demographic
clinical
computerized patient charting database was used to collect:
Treatment course data
Process measures
Audiologist recommendations
The study was a retrospective descriptive analysis. The authors determined audiologic, demographic, and clinical features of the pediatric patients. A computerized patient chart database was used to collect Tx course data, process measures, and audiologist recommendations. The study was a retrospective descriptive analysis. The authors determined audiologic, demographic, and clinical features of the pediatric patients. A computerized patient chart database was used to collect Tx course data, process measures, and audiologist recommendations.
14. Audiologist Recommendations Hearing Aid
Makes certain sounds louder
Programming is based on individual�s freq specific hearing thresholds
Limitations
Output (especially in the high freqs)
FM system
Ideal for children with minimal hearing loss
Most often used in classroom setting only The audiologist recommendations that the authors considered were hearing aids or FM system use. Both technologies are available for people with hearing loss and they provide access to sounds that the person would not hear without the devices. These types of technology are a vital part of the child�s education. Without use of hearing aids, cochlear implants, or other assistive listening devices, many children with hearing loss are not able to develop appropriate language skills, often leading to poor academic outcomes.
Hearing aids are a type of personal amplification system, which are fit specifically based on an individual�s needs (audiogram). Hearing aids provide volume, or gain, in specific frequency regions that a person is not able to hear without amplification. There are various types and styles of hearing aids. An audiologist is a hearing professional that prescribes, fits, and manages hearing aids and other types of assistive devices. The earlier a child is fit with hearing aids, the better. Late identification of hearing loss or a delay in intervention services often result in delayed speech and language development.
FM systems work like small radios. There is a microphone that picks up the teachers voice and the child receives the signal directly to their ears or desk top, alleviating the problems that noise could potentially cause on a child with hearing loss. This type of device is often used in children with minimal hearing loss, just to ensure that environmental noises are not masking out the intended signal. FM systems can be used in classrooms, in the car, and even at home.
The audiologist recommendations that the authors considered were hearing aids or FM system use. Both technologies are available for people with hearing loss and they provide access to sounds that the person would not hear without the devices. These types of technology are a vital part of the child�s education. Without use of hearing aids, cochlear implants, or other assistive listening devices, many children with hearing loss are not able to develop appropriate language skills, often leading to poor academic outcomes.
Hearing aids are a type of personal amplification system, which are fit specifically based on an individual�s needs (audiogram). Hearing aids provide volume, or gain, in specific frequency regions that a person is not able to hear without amplification. There are various types and styles of hearing aids. An audiologist is a hearing professional that prescribes, fits, and manages hearing aids and other types of assistive devices. The earlier a child is fit with hearing aids, the better. Late identification of hearing loss or a delay in intervention services often result in delayed speech and language development.
FM systems work like small radios. There is a microphone that picks up the teachers voice and the child receives the signal directly to their ears or desk top, alleviating the problems that noise could potentially cause on a child with hearing loss. This type of device is often used in children with minimal hearing loss, just to ensure that environmental noises are not masking out the intended signal. FM systems can be used in classrooms, in the car, and even at home.
15. Audiologic Grading Serial behavioral audiograms (ear specific in all but 7 patients)
Audiograms were graded in a blinded manner (w/out knowledge of tx regimen or clinical hx)
All audiograms assigned CTCAE, Brock, & Chang grades.
16. Audiologic Grading Continued CTCAE subjective criteria were not used in order to keep the grading blinded
HL at 25-90 dB was averaged at 3 contiguous frequencies
Chang grading scale � modified version of Brock scale
Meant to incorporate functional deficits caused by HL < 40dB
17. Chang vs Brock The chang grading scale takes into account lesser degrees of hearing loss and establishes a more specific range of possible deficit. The chang grading scale takes into account lesser degrees of hearing loss and establishes a more specific range of possible deficit.
18. This is an example of one audiogram and the grade that would be assigned based on the grading scale used.This is an example of one audiogram and the grade that would be assigned based on the grading scale used.
19. Data Analysis Linear regression
Used to test the relationship between audiogram-based ototoxicity grades and the following factors:
Delivery volume
Mannitol usage
Dextrose usage
Tx length
Cumulative and daily cisplatin dosage
Patient age
patient body-surface area (BSA)
20. Data Analysis continued One-tailed, two-sample Mann-Whitney U test was used to assess mannitol usage, comorbidity, radiotherapy coadministration, and metastatic status.
Pearson x squared values were used to test the interaction btwn audiogram-based ototoxicity grades and the final recommendations made by audiologists Mannitol used w/ chemotherapy to prevent kidney damage. Metastatis is when cancer travels from the original site within the body to another location. Mannitol used w/ chemotherapy to prevent kidney damage. Metastatis is when cancer travels from the original site within the body to another location.
21. Results
No significant difference in mean grade among the different diagnoses (P=.357), using univariate analysis of variance.
Patients with higher Chang grades had higher chance of requiring a HA or FM system
22. Results: Demographics & Clinical Characteristics
23. Results continued Children with higher Chang grades were recommended to receive intervention. Patients with grades 2b and 3 tended to be younger with smaller BSA.Children with higher Chang grades were recommended to receive intervention. Patients with grades 2b and 3 tended to be younger with smaller BSA.
24. Results continued The grade distribution of patients receiving cisplating and carboplatin is summarized in Figure 2. The 67 patients receiving cisplatin as their only primary ototoxic chemotherapeutic agent had average grade of .8 compared with .2 in the 9 patients receiving only carboplatin (p=.031, Man-Whitney). Only one of the carboplatin patients had a grade higher than 0. Patients receiving only carboplatin had a lesser grade despite the fact that they were younger than the cisplatin-only group (men age, 1.1 v 11.4 years, respectively). The 14 patients receiving both agents had a higher average grade (1.2) compared with patients in the other 2 groups. The grade distribution of patients receiving cisplating and carboplatin is summarized in Figure 2. The 67 patients receiving cisplatin as their only primary ototoxic chemotherapeutic agent had average grade of .8 compared with .2 in the 9 patients receiving only carboplatin (p=.031, Man-Whitney). Only one of the carboplatin patients had a grade higher than 0. Patients receiving only carboplatin had a lesser grade despite the fact that they were younger than the cisplatin-only group (men age, 1.1 v 11.4 years, respectively). The 14 patients receiving both agents had a higher average grade (1.2) compared with patients in the other 2 groups.
25. Results continued The table here illustrates how the Chang and CTCAE grades from audiogram scoring were significantly related to the audiologist recommendations regarding hearing aid or FM system (p< .0001, pearson x squared). The chang scale was more specific though, with the CTCAE scale diverging from therapeutic recommendations at higher grades as seen in the table. The CTCAE scale was not specific in determining hearing aid use. The table here illustrates how the Chang and CTCAE grades from audiogram scoring were significantly related to the audiologist recommendations regarding hearing aid or FM system (p< .0001, pearson x squared). The chang scale was more specific though, with the CTCAE scale diverging from therapeutic recommendations at higher grades as seen in the table. The CTCAE scale was not specific in determining hearing aid use.
26. Take home message Both the Chang and CTCAE grades from audiogram scoring were significantly related to the audiologists� recommendations (FM or HA use)
Chang scale was more specific than the CTCAE scale
Patients receiving combination radiation therapy, lower BSA, and patients with metastatic disease had higher grades
27. Limitations of the Study Retrospective analysis
Ear specific data not available on each patient
More treatment options besides FM systems and hearing aids
Audiologist recommendations are based on various factors
Uneven comparison groups
28. Clinical Considerations/Use Audiologist can report a grade versus a lengthy descriptive analysis
Promotes interspecialty communication re: ototoxic clinical effects
Modifications to tx protocols when applicable
Helps with counseling families/patients
Grading system is practical and easy to interpret
29. Future research Prospective analysis
Use of a specific audiology test protocol
Test high frequencies only, interfrequencies
Establish specific audiology recommendations based on objective data
More balanced groups
Mannitol � possible otoprotectant?
Randomized controlled study
In the study, patients who received higher levels of mannitol had lesser degrees of hearing lossIn the study, patients who received higher levels of mannitol had lesser degrees of hearing loss