Download
1 / 28
280 likes | 342 Vues
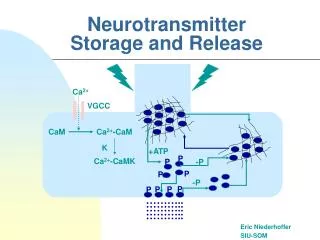
Neurotransmitter Release: exocytosis and endocytosis. Transmitter synthesized and stored Action Potential Depolarization: open voltage-gated Ca 2+ channels Ca 2+ enter cell Ca 2+ causes vesicles to fuse with membrane Neurotransmitter released (exocytosis)

E N D
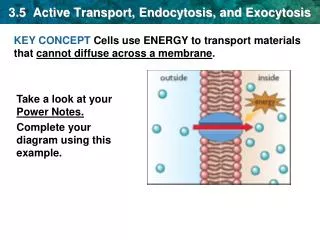
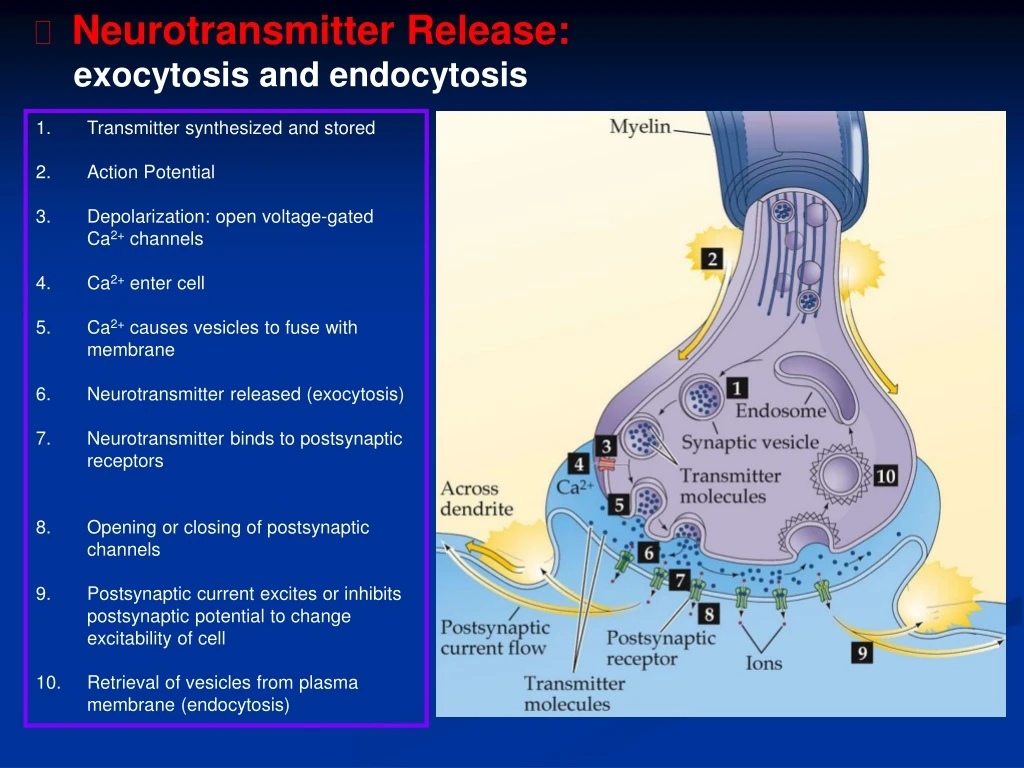
Neurotransmitter Release: exocytosis and endocytosis Transmitter synthesized and stored Action Potential Depolarization: open voltage-gated Ca2+ channels Ca2+ enter cell Ca2+ causes vesicles to fuse with membrane Neurotransmitter released (exocytosis) Neurotransmitter binds to postsynaptic receptors Opening or closing of postsynaptic channels Postsynaptic current excites or inhibits postsynaptic potential to change excitability of cell Retrieval of vesicles from plasma membrane (endocytosis)
Transmitter Inactivation: reuptake and enzymatic breakdown Reuptake by transporters (glial cells) Reuptake by transporters Enzymatic breakdown Neurotransmitter can be recycled in presynaptic terminal or can be broken down by enzymes within the cell
NT – Receptor Binding Receptors are large, dynamic proteins that exist along and within the cell membrane. Dynamic – they can increase in number and avidity for their neurotransmitter according to circumstances. Two Types of Post synaptic Receptors: Ionotropic receptors: NT binding results in direct opening of specific ion channels Metabotropic receptors: binding of NT initiates a sequence of internal molecular events which in turn open specific ion channels
Ionotropic Receptors Work very fast; important role in fast neurotransmission Each is made of several subunits (together form the complete receptor) At center of receptors is channel or pore to allow flow of ions At rest - receptor channels are closed When neurotransmitter binds -- channel immediately opens When ligand leaves binding site -- channel quickly closes
Metabotropic Receptors… Work by activating other proteins called G proteins Each is made of several transmembrane regions Stimulate or inhibit the opening of ion channels in the cell membrane Work more slowly than ionotrophic receptors
Metabotropic Receptors… Stimulate or inhibit certain effector enzymes Most effector enzymes controlled by G proteins are involved in synthesis of second messengers. *First messenger: ligand. *Second messenger: effector enzyme
Second messengers: Activate Protein Kinases Can work by affecting: NT production, no. synapses formed, sensitivity of receptors, or expression of genes (long term effects). Can result in amplification - interconnections.
Other Metabotropic Receptors Work more slowly than ionotropic receptors Though it takes longer for postsynapic cell to respond, response is somewhat longer-lasting Comprise a single protein subunit, winding back-and-forth through cell membrane seven times (transmembrane domains) They do not possess a channel or pore
Tyrosine Kinase Receptors: TrkA: NGF TrkB: BDNF and NT-4 TrkC: NT-4
Receptors superfamilies: • Ionotropic receptors (ligand-gated channels) • Metabotropic receptors (G protein-coupled receptors) • Tyrosine Kinase Almost all neurotransmitters discovered so far have more than one kind of receptor -- called receptor subtypes.
Receptors are dynamic • Large and prolonged intake of certain substances cause an increase in the number of receptors (basis of withdrawal response in addiction). • Each NT influences its own receptors independent of the action of other receptors. • Excitatory and inhibitory NTs. • Post-synaptic neuron sums up the influences of all NTs. • “All or nothing” response (must reach threshold to fire).
Receptors provide for temporal flexibility (ms to decades) • Multiple types of receptors exist for each major family of NT receptors. • Example: serotonin – at least 14 subtypes exist based on potency of binding to different drugs. - Imitrix for migraines - Prozac for depression Affect different serotonin subtypes. ■ Can develop drugs to target very specific receptors. ■ Provides for much variety and subtlety of response in the human brain.
Richard Restak, MD, PhD • “The brain as a whole can be understood as the summation of billions of interacting neurons influencing one another via the interplay of hundreds of neurotransmitters and their receptors, which in turn influence the passage of electrically charged particles across the nerve cell membrane.”
Pharmacology of Synaptic Transmission Drugs affect synaptic transmission in many different ways. They can act as agonists or antagonists.
Synapses are targets for many recreational drugs amphetamine* cocaine phencyclidine nicotine neurotransmitter transporters neurotransmitter-activated channels postsynaptic cell G protein coupled receptors enzymes G protein-activated channels N C a LSD morphine-heroin tetrahydrocannabinol caffeine ?alcohol?
Nicotine • Nicotine mimics acetylcholine at its receptor site. • Called cholinergic or “nicotinic” receptor. • Especially effective within the areas of the limbic system involved in the pleasure response. • Prevents transmission of impulses at NM junctions. • Evolved with plants to protect against insects (insecticide). • Banded krait (Malayan snake) kills its prey by attacking the NM junction (paralyzes prey).
Nicotine experiment – Keller and Schwartz • Gave radioactively labeled nicotine to rats. • Found > number of nicotinic receptors vs. controls. • Unusual – receptors usually ↑ in numbers when there is a shortage of stimulation. • Solution: nicotine initially exerts a stimulatory effect (agonist), and then desensitizes receptors to render them nonfunctional for long periods. • This stimulates the neurons to produce more receptors.
Nicotine’s Appeal • Nicotine in the brain causes release of a wide variety of NTs, including endorphins, and dopamine (pleasure). • Anxiety-reducing effects. • Lessening of irritation and aggression, suppression of appetite (loss of weight). • With repeated smoking, these effects diminish – the brain becomes tolerant to nicotine. • Smoker smokes more → dependence.
Nicotine Addiction • Brain has modified its functioning in response to regular nicotine “hits”. • Smoker attempts to cut down – craving due to events at nicotinic-acetylcholine receptors. • Withdrawal: irritability, frustration, anger, anxiety, difficulty concentrating, restlessness, decreased heart rate, increased appetite and/or weight gain. • 70-80% of people who try to quit smoking relapse within one year.
Is nicotine a “bad” drug or a “good” drug? • Alzheimer’s disease – dramatically reduced number of cerebral nicotinic receptors. • Could prescribe nicotine to increase receptors. • Problems: ethical considerations, possible unknown side effects, much testing to be done. • “At the level of the neuron there are no good or bad drugs, only drugs that alter the brain.” • Social and economic factors play a role.
Caffeine – “good” or “bad”? • Caffeine ingestion is almost universal. • Leads to activation of cerebral cortex (EEG). • Most helpful when a person is already tired. • Caffeine blocks the brain’s receptors for adenosine, an inhibitory NT (inhibits release of excitatory NTs) • Leads to stimulation, alertness, and an elevation of mood.
Caffeine – the “bad” • Too much – restlessness, difficulty composing thoughts, vertigo, headaches, agitation, and an irregular heartbeat. • Withdrawal – headache, irritability, restlessness, and drowsiness. • Headache due to caffeine’s ability to constrict BVs that feed the brain and scalp. • Withdraw caffeine – vasodilation → headache. • Addicting
Caffeine – the “good”? • Many over-the-counter headache remedies contain caffeine. • Caffeine’s actions resemble those of amphetamines – fatigue disappears, mood improves, and sociability is enhanced. • It is very likely that new substances will be synthesized in the future that have similar desirable effects. • Would these developments alter our tendency to put judgmental labels on commonly used substances that act on the brain?
“Angel Dust”, a.k.a. PCP • Phencyclidine was first developed as an anesthetic – no apparent side effects in animals. • Humans – 15% showed marked confusion, violence, and psychotic behavior as in schizophrenia. • Became a popular street drug in the 1960’s. • At the same time, researchers were carrying out non-FDA approved experiments using PCP as a “facilitator” for psychotherapy. • Also used as a “model” for schizophrenia.
PCP Side Effects • Low dose – induced a state resembling drunkenness. • Larger doses – person felt no pain (analgesic effect). • High doses – patient acted schizophrenic – effects lasted about 4 hours. • Afterwards – depression, paranoia, and sometimes suicidal or homicidal behavior. • Highest doses – epileptic convulsions, respiratory depression, and death. • Users found that bad effects could be reduced by smoking rather than ingesting the drug.
PCP – the “good” • In 1981, neuroscientists discovered a PCP receptor in the brain. • Hypothesis: PCP might be acting at the same sites in the brain responsible for schizophrenia. • Couldn’t confirm or disprove this hypothesis. • However, this lead to many other discoveries that revolutionized treatment for stroke and other destructive brain injuries (excitotoxic theory – glutamate).
Synapses are the targets of therapeutic drugs • Antidepressant drugs • serotonin uptake inhibitors • Analgesics (morphine) • opiate receptor agonists • Antipsychotic drugs • DA receptor antagonists • Anticonvulsant drugs • GABAA modulators • Antianxiety agents • GABAA modulators