Download
1 / 12
131 likes | 250 Vues
Benefits in Health Insurance: Calculating the Costs and Premiums. Alliance for Health Reform October 10, 2008 John Bertko, FSA, MAAA. Calculation of Health Insurance Premiums . For $1 in premium, on average across all markets: 85¢ for claims/services

E N D
Benefits in Health Insurance:Calculating the Costs and Premiums Alliance for Health Reform October 10, 2008 John Bertko, FSA, MAAA
Calculation of Health Insurance Premiums • For $1 in premium, on average across all markets: • 85¢ for claims/services • 10¢ for administration (marketing, billing and enrollment, claims adjudication, network management, care coordination) • 5¢ for profits or contribution to surplus (for non-profits) [Note that this allocation of a premium dollar varies by market, by region, by calendar year and by company.]
Benefit Plan Design • Defining what level of benefits is regarded as adequate • Affordability -- a trade-off between cost-sharing and premium cost • Cost-sharing -- includes deductibles, coinsurance, copays and out-of-pocket maximum • More cost-sharing reduces premium and utilization • RAND Health Insurance Experiment (HIE) showed that most individuals reduced services used without effects on health • Exception for those in poor health • Can devise designs that have lower cost-sharing for: • Primary care office visits • Screening • Preventive services • What is the minimum benefit?
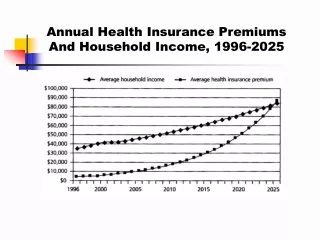
Benefit Design and Premiums • Premiums • Vary by geographic region, age and level of benefits • Based on: • Population -- e.g., for non-Medicare age adults • Allowed charges (contracted provider rates) • Expected utilization (by age, industry, health status) • Network used (“narrow” network for HMOs vs. tiered networks vs. “wide” PPO networks) • Utilization management (e.g., prior authorization, step therapy, etc.) • Reduced for cost-sharing
Benefit Plans • Which design to use as a starting point? • FEHBP’s BCBS Standard Plan -- a relatively high level of benefits ($300 deductible PPO) • Medicare (without supplemental Medigap) • $1024 Hospital per admission deductible in 2008 • $135 separate Part B deductible in 2008, plus 20% coinsurance • No Out-of-Pocket cap on cost-sharing • Average benefit plan purchased by employers • Typically higher deductible PPO • ~$500 deductible for large employers • Range from $500 to $2500 for small employers • Range from $1000 to $5000 for individuals • HMO vs. PPO: tradeoffs between smaller provider network and lower premiums • Indexing -- at what rate should cost-sharing change each year?
Benefit Plans • Actuarial Equivalence -- average cost-sharing is the same • E.g., deductibles+coinsurance may be equivalent to copays+per admission cost-sharing • Determined by using costs for an “average individual” from a specific population (e.g., adults 18-64), • Equivalent plans must cover the same services (e.g., hospital, physician, prescription drugs) • Cost sharing for individuals with different health needs will vary • Actual premiums will vary across insurers for actuarially equivalent benefit designs • Actuarial equivalence can be used to allow variation in benefits while guaranteeing compliance with minimum benefit plan rules • Part D uses this standard
Model Plan $300 deductible 80% in network payment 60% out-of-network payments $2500 maximum out-of pocket Actuarially equivalent plan $20 Primary Care copay in network $50 Specialist copay in network $100 Emerg Room copay 50% coinsurance out-of-network $250 per admission deductible Rx: $10/20/50/25% copays/coinsurance $2500 maximum out-of-pocket Example of Actuarial Equivalence
Limits on Rate Variation • Same $$s need to be collected • Adjusted Community Rating • Vary by age, gender, location, benefit design and network • No variation for health status • Healthy subsidize the less healthy at the same age
Limits on Rate Variation • Rate bands • Small Group regulation • “Manual rates” vary with case characteristics like age, gender, number of employees, location • With health status or industry, rates may further vary by (e.g., NAIC model) +/- 35% • Many differences across the states • Most common rate band is +/- 25%
Limits on Rate Variation • Underwritten rates in Individual market • Three main underwriting outcomes: • Standard rate offers for the healthy • Less than rates for “average employees” or dependents since these Individuals are healthy at policy issue • Rate-ups or pre-ex offers of insurance • Rate-ups will be from 110% to 200% of standard • Pre-ex offer may have same rate, but limits on covered conditions • Denials -- no offer made • Possible use of High Risk Pools
Limits on Rate Variation • High Risk Pools • Rates are generally 200% to 250% of standard rates • HRP capacity for enrollees is constrained by funding from: • Assessments on insured policies • Other sources (e.g., tobacco taxes)
More Technical Topics • Adjusted Community Rating changes to market premiums • Use of Reinsurance • Effects of Guaranteed Issue • Effects on premiums of individual or employer mandates • Effects of Risk Adjustment