Download
1 / 65
760 likes | 1.53k Vues
In Situ Carcinoma of the Breast. Kiwhoon Lee, M.D. Department of Radiation Oncology Multi-Modality Conference May 27, 2010. Overview. Definition and Anatomy Histopathology and Biology Epidemiology and Etiology Treatment Options Prospective Studies Conclusions. Definition of DCIS.

E N D
In Situ Carcinoma of the Breast Kiwhoon Lee, M.D. Department of Radiation Oncology Multi-Modality Conference May 27, 2010
Overview • Definition and Anatomy • Histopathology and Biology • Epidemiology and Etiology • Treatment Options • Prospective Studies • Conclusions
Definition of DCIS • Pathologic definition • Clonal proliferation of cells that appear malignant and that accumulate within the lumen of the mammary duct without evidence of invasion beyond the epithelial basement membrane into the adjacent breast stroma • Descriptive and synonymous terms • Noninvasive • Stage 0 (Tis DCIS) • Preinvasive Burstein N Engl J Med 2004
Proliferative Breast Disease • Normal Terminal Duct Lobular Unit • Epithelial Hyperplasia • Atypical Ductal Hyperplasia Robbins Pathological Basis of Disease – 6th ed.
Relative Risk for Invasive Carcinoma • Hyperplasia – moderate or florid sclerosing adenosis, papilloma • Slighty increased risk (1.5-2 times) • ADH and ALH • Moderately increased risk (4-5 times) • DCIS • High risk (8-10 times) Hutter Arch Pathol Lab Med 1986 110:171-3
Distinction Between ADH & DCIS • Difficult to distinguish DCIS from Hyperplasia or Atypical Hyperplasia • Various degrees of cellular and architectural atypia • Greater cellular homogeneity with nuclear hyperchromasia, architectural uniformity, and more extensive distribution favor DCIS
Distinction Between ADH & DCIS • Rosai J. Am J Surg. Path. 1991: 15; 209-221 • 5 internationally acclaimed pathologists • Not a single case (10 cases) in which all agreed • Only 2 (20%) cases in which 4/5 agreed • 4 cases (40%) in which diagnosis spanned all three types of lesions
Histopathologic Evaluation • Extent (multifocal or multicentric) • Size • Grade (High vs. Low) • Subtype & necrosis • Calcifications • DCIS in non-calcified areas • Invasion or microinvasion • Margins (+ or -) Extent of negative margin
Estimating Size of DCIS • Difficult to measure because it is usually nonpalpable and cannot be identified grossly • Several pathologic methods: • Direct measurement if confined to a single slide • Microscopic exam of entire specimen in sequence and in sections of uniform thickness (2 to 3 mm) • Estimating percentage of breast tissue involved by DCIS in relation to total specimen • Reporting number of slides & number with DCIS • Surgical margin accuracy dependent on a detailed examination of entire specimen • Direct measurement of calcifications on mammogram
Subtypes of DCIS • Comedo • Non-comedo • Cribriform • Micropapillary • Papillary • Solid
Comedocarcinoma Robbins Pathological Basis of Disease – 6th ed.
Non-comedo DCIS Solid DCIS Low-grade cribriform DCIS with microcalcifications Papillary DCIS Micropapillary DCIS (left) and comedocarcinoma (right) Robbins Pathological Basis of Disease – 6th ed.
Biology of DCIS Low GradeHigh Grade ER+ Frequent Infrequent PR+ Frequent Infrequent C-Erb Infrequent Frequent (Her-2 Neu) P-53 Infrequent Frequent Ki-67 Ab Infrequent Frequent Bobrow LG et al. Sem. Diag. Path., 1994: 11; 199-207 Zafrani B et al. Sem Diag. Path., 1994: 11; 208-214
Progression to Invasion • Nearly all invasive breast cancers arise from in situ carcinomas • Clonal evolutionary relationship • Shared chromosomal changes in both DCIS and synchronous, adjacent invasive cancers Stratton J Pathol 1995 Radford Cancer Res 1995
Natural History • Page et al. • 28 women small, noncomedo ductal carcinomas in situ excised by biopsy only • Median follow-up ~30 years • Overall risk of invasive carcinoma is 9 times that of general population (95% CI: 4.7-17) • All invasive carcinomas developed in the same area of the same breast Page Cancer 1995
DCIS Incidence Rates Age (Years) 1974 1992 30 - 39 2/100,000 5/100,000 40 - 49 5/100,000 28/100,000 50 + 7/100,000 45/100,000 NCI SEER (Ernster, JAMA 1996; 275: 12)
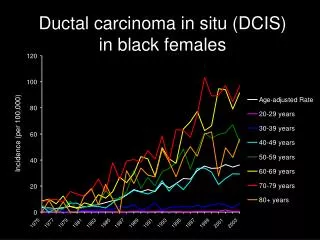
DCIS Incidence Rates Age-adjusted incidence of ductal carcinoma in situ (DCIS) per 100 000 women over time, adjusted to age distribution of women 18 years old or older in the 2000 U.S. Census Baxter, N. N. et al. J Natl Cancer Inst 2004;96:443-448
Changing Presentation of Breast Cancer YearsAvg. SizeInv. Ca. > 3 NDCIS 1969-73 2.5 cm 17% 3% 1974-78 2.4 cm 18% 4% 1979-84 2.0 cm 14% 3% 1985-88 2.0 cm 11% 11% 1989-93 1.5 cm 10% 14% Cady et al. Arch Surg. 1996; 131: 301-308 and NCI SEER (Ernster, 1996)
Epidemiology • 15% - 20% of all breast cancers • 35% - 40% of all mammographically detected breast cancer • 1 in 1300 screening mammograms • Data on the course of progression of DCIS to invasion, if untreated, is not well known • Early detection results is very high breast cancer free survival rates NCI SEER (Ernster JAMA 1996)
Diagnostic Work-up • History and Physical • Diagnostic mammogram • Craniocaudal and mediolateral oblique views • Magnified views/Spot Views • Stereotactic core-needle biopsy • Needle-localized wide excision • Specimen radiograph to confirm sampling • Post-excision mammogram
Clinical Presentation • Mammographic abnormalities (most common) • Microcalcifications
Mammography Note linear-branching calcifications extending along the ducts toward the nipple
Stereotactic Needle Biopsy • One of two instruments used: • Core Needle • Vacuum assisted device
Stereotactic Needle-Localization • Needle should transfix lesion • Confirm w/ CC and MLO views • Needle is placed 1 cm passed lesion • Due to “accordion effect” • Wire is placed near abnormal area
Treatment Options • Mastectomy • Wide Local Excision ( “Lumpectomy”) • Excision alone (with negative margins) followed by observation only (no RT) • Carefully selected patients • Excision followed by RT • WBI • APBI • Role of Tamoxifen post treatment
Treatment History of DCIS in United States YearCasesMast.Exc.Exc.+RTNo Surg 1983 4900 71% 19% 6% 4% 1988 17217 58% 26% 14% 2% 1992 23368 44% 30% 23% 3% 1999 25206 28% 32% 38% 2% Ernster VL et al. JAMA 1996; 275: 913-918 Baxter, N. N. et al. J Natl Cancer Inst 2004;96:443-448t
Mastectomy • Historical standard of treatment • Great local control and overall survival • Suggested Indications: • Multifocal or multicentric DCIS • Diffuse, malignant appearing microcalcifications • Persistent positive margins after surgical attempts • Other: small breast, unable to have RT, etc. Winchester DP. CA Cancer J Clin 1998: 48; 108 - 128
Mastectomy • Overall survival (OS) and local failure (LF) rates are excellent at 96 - 100% and 0 - 1% Study # LF(%) OS(%) F/U (yrs.) Fisher, E. 28 0% 96% 3.2 Lagios 98 0% 100% Silverstein 228 1% 100% 6.7 Temple 116 0% 100% 7.5 • Overtreatment? Poor cosmesis and psychological factors
Breast Conservation Therapy • 3 randomized trials • NSABP B-17 • EORTC • UKCCR
NSABP B-17 Prospective randomized trial:Fisher B Semin Oncol 2001 • 818 patients randomized to lumpectomy vs. lumpectomy + XRT • Stratified by age (≤49yrs or >49 yrs), tumor type, and method of detection (clinical or mammographic) • All patients with negative margins were eligible • Tumor size groups evaluated: <0.1 cm, 0.1-1.0 cm, 1.1-2.0 cm and >2.0 cm; all determined pathologically (median # of sections was 8-10) • 50 Gy given using tangents ≤ 8 wks after surgery • 12 year update
At 12 years of follow-up: LFLump. + RTLump. DCIS 8% 14.6% Invasive 7.7% 16.8% Total 15.7% 31.4% Fisher, B. Semin Oncol. 2001 Aug; 28(4):400-18
Follow-up pathologic review (573/790 Pts.): • Lumpectomy (391 Pts.) vs. Lumpectomy + RT (399 Pts.) • Recurrence rates (%): LumpectomyLump. + RT Comedo (-) 9.3 4.8 Comedo (+) 19.5 5.3 Margins (-) 11.2 4.0 Margins (+) 25.4 10.0 Size (< 1 cm) 13.5 5.3 Size (> 1 cm) 18.8 3.2 Fisher, E. R Cancer 1995; 75:1310-9
NSABP B-17 IBTR (%) 5 yr 8 yr 12 yr Excision alone 16 27 32 Excision + XRT 7 12 16 p<0.001
NSABP B-17 Conclusions • In patients with negative margins, RT reduces risk of ipsilateral noninvasive and invasive recurrences by >50% • Margin status and comedo necrosis are independent predictors of recurrence • If margins are negative, RT erases comedo variable • RT did not affect overall survival
EORTC 10853 Prospective randomized trial: Julien, J.P. et al The Lancet 2000; 355: 528-533 Bijker, N et al, JCO 2006; 24:3381-3387 (10 yr update) • Design similar to NSABP B-17 • 1010 patients randomized to wide local excision (n=503) vs. wide local excision + XRT (n=507) • All eligible patients with negative margins • Tumor size <5 cm eligible, determined clinically or via extent of microcalcifications on mammography • 50 Gy in 25 fractions using medial/lateral tangents • Median follow-up = 10.5 years
EORTC 10853 Results At 10 years of follow-up: ExcisionExcision + XRT Local recurrence 26% 15% Event-free survival 70% 76% • ~50% reductions in both DCIS and invasive breast recurrences by radiotherapy • Risk factors on multivariate analysis: Age, Method of detection, Histologic type, Architecture, Margins, and Treatment P=0.005
UKCCCR • Prospective randomized trial – UK, New Zealand, and Australia • 2-by-2 factorial design to randomize 1701 pts after lumpectomy for DCIS: • Radiotherapy or not • Tamoxifen or not • Median f/u = 52.6 mo
UKCCCR Results Houghton Lancet 2003
Indication for TamoxifenNSABP B-24 • Prospective randomized trial • 1804 pts treated with BCS + RT (50 Gy) per B-17 • Placebo vs Tamoxifen • Allowed diffuse calcifications and positive margins Fisher, B. Lancet 1999: 353; 1993-2000
Conclusions of NSABP B-24 • Women treated with lumpectomy + RT showed additional benefit when treated with tamoxifen and tamoxifen decreased both ipsilateral and contralateral breast cancer recurrences • Minimal increase in endometrial carcinoma • Mastectomy can be more frequently avoided Fisher Lancet 1999
Excision Alone Author#5yr LF(%)10yr LF(%)Inv. (%) Arnesson 169 16% 22% 36% Fisher, B. 403 22% 27%(8y)/32%(12y) 50% Lagios 79 12% 19% 56% Schwartz 194 14% 25% 18% Silverstein 130 20% 22% 33% Winchester DP et al. CA Cancer J Clin 1998: 48; 108 - • Risk for invasive recurrence (~ 10%) @ 5 yrs.
Influence of Margins • Silverstein (1999): N=469 pts • Local recurrence @ 8 yrs: Margin WidthNo RTWith RTRecommend > 10 mm 3% 4% WLE alone 1 - 10 mm 20% 12% WLE+/- RT < 1 mm 58% 30% WLE + RT • Criticisms • Need complete tissue processing • Retrospective, non-randomized study Silverstein N Engl J Med 1999
Recurrences in 133 Patients with Ductal Carcinoma in Situ and Excision Margins at Least 10 mm Wide Silverstein, M. J. et al. N Engl J Med 1999;340:1455-1461
Recurrences in 224 Patients with Ductal Carcinoma in Situ and Excision Margins 1 to <10 mm Silverstein, M. J. et al. N Engl J Med 1999;340:1455-1461