Download
1 / 25
290 likes | 716 Vues
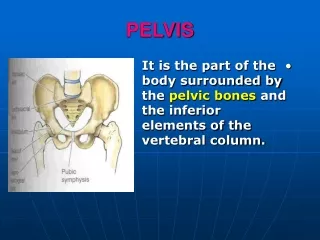
CLINICAL ANATOMY OF THE. PELVIS. Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday. Male Pelvis v.s. Female Pelvis. Sexual differences are related mainly Heavier build and larger muscles of most men Adaptation of the pelvis (particularly the lesser pelvis)

E N D
CLINICAL ANATOMY OF THE PELVIS Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday
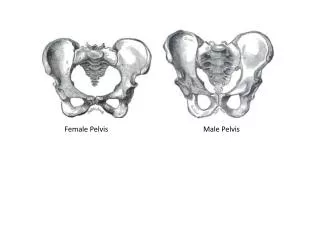
Male Pelvis v.s. Female Pelvis Sexual differences are related mainly Heavier build and larger muscles of most men Adaptation of the pelvis (particularly the lesser pelvis) in women for parturition (childbearing). The difference between the male and female pelvis Difference Between Male & Female Pelvis
male or funnel-shaped pelvis with a contracted outlet long, narrow, and oval shaped 41% of women widepelvis 2% of women
In forensic medicine (the application of medical and anatomical knowledge for the purposes of law), identification of human skeletal remains usually involves the diagnosis of sex. • A prime focus of attention is the pelvic girdle because sexual differences usually are clearly visible. • Even fragments of the pelvic girdle are useful in determining sex.
PELVIC DIAMETERS (CONJUGATES) Size of the lesser pelvis important in obstetrics Because it is the bony canal through which the fetus passes during a vaginal birth. To determine the capacity of the female pelvis for childbearing, diameters of the lesser pelvis are noted radiographically or manually during a pelvic examination.
Antero - posteriordiameters • Diameters of pelvicoutlet Anatomicalantero-posterior diameter11cm fromtip of the coccyx tolowerborder of symphysispubis Obstetric antero-posterior diameter13 cm fromtip of the sacrum tolowerborder of symphysis pubis as the coccyx moves backwards during the second stage of labour.
Transversediameters • Diameters of pelvicoutlet Bituberousdiameter11 cm betweeninneraspects of ischialtuberosities Bispinousdiameter10.5 cm betweentips of ischialspines
Diameters of pelvicinlet Antero - posteriordiameters Anatomicalantero-posteriordiameterTrue conjugate11cm fromtip of sacralpromontorytoupperborder of symphysispubis
Diameters of pelvicinlet Antero - posteriordiameters Obstetricconjugate10.5 cm fromtip of sacralpromontory to themostbulging point on backof symphysis pubis,about1 cm below its upper border. shortestantero-posteriordiameter
Diameters of pelvicinlet Antero - posteriordiameters Diagonalconjugate12.5 cm 1.5 cm longer than the trueconjugate Fromtip of sacral promontory tolowerborder of symphysispubis
Minimum anteroposterior (AP) diameter of the lesser pelvis True (obstetrical) conjugate Narrowest distance through which the baby's head must pass in a vaginal delivery. This distance, however, cannot be measured directly during a pelvic examination because of the presence of the bladder.
Diagonal conjugate (from inferior pubic lig. to promontory) Measured by palpating sacral promontory with the tip of the middle finger, using the other hand to mark the level of the inferior margin of the pubic symphysis on the examining hand. After the examining hand is withdrawn, the distance between the tip of the index finger (1.5 cm shorter than the middle finger) and the marked level of the pubic symphysis is measured to estimate the true conjugate, which should be 11.0 cm or greater.
Transverse diameter is the greatest distance between the linea terminalis on either side of the pelvis.
Pelvic Fractures • Anteroposterior compression of the pelvis occurs during crush accidents (as when a heavy object falls on the pelvis). • This type of trauma commonly produces fractures of the pubic rami. • When the pelvis is compressed laterally, the acetabula and ilia are squeezed toward each other and may be broken.
Fractures of the bony pelvic ring are almost always multiple fractures or a fracture combined with a joint dislocation. Pelvic fractures can result from direct trauma to the pelvic bones, such as occurs during an automobile accident, or be caused by forces transmitted to these bones from the lower limbs during falls on the feet.
Weak areas of the pelvis, where fractures often occur: Pubic rami Acetabula Region of the sacroiliac joints Alae of the ilium 25 Year Old Male with displaced fracture of the sacrum andsymphysis pubis. The most severe pelvic fractures separate the two sides of the pelvis from each other.
Pelvic fractures may cause injury to pelvic soft tissues, blood vessels, nerves, and organs. Fractures in the pubo-obturator area are relatively common and are often complicated because of their relationship to the urinary bladder and urethra, which may be ruptured or torn.
Sacroiliac joint dysfunction Degenerativearthritis (osteoarthritis) Pregnancy Gout Rheumatoid arthritis Psoriasis Ankylosingspondylitis X-ray of the sacroiliac joints showing joint space narrowing, erosive change and indistinct margins, due to sacroiliitis