Download
1 / 30
300 likes | 317 Vues
Risk Factors for Delayed Vaccine Uptake Among Children in Kumasi. Joshua Arthur 1 , Fred Kwame Awittor 2 , Nicholas Karikari-Mensah 3 , Dennis Odai Laryea 1

E N D
Risk Factors for Delayed Vaccine Uptake Among Children in Kumasi Joshua Arthur1, Fred Kwame Awittor2, Nicholas Karikari-Mensah3, Dennis Odai Laryea1 1: Public Health Unit, Komfo Anokye Teaching Hospital, Kumasi; 2: Non-Communicable Disease Surveillance Section, Public Health Unit, KATH, Kumasi; 3: Communicable Disease Surveillance Section, Public Health Unit, KATH, Kumasi
Outline • Background • Objective • Methods • Results • Conclusion • Recommendations
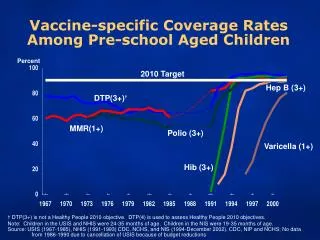
Background • Decline in vaccine-preventable illnesses one of the most significant public health achievements in the past century • Childhood immunisation identified as one of the most cost effective health interventions1,2 • An estimated 35 billion dollars be spent on immunisations between 2006 and 20153 • Overall, an estimated 2-3 million deaths averted per annum through immunisation4 1Coffield et al, 2001; 2Miller et al, 2004; 3Wolfson et al, 2008; 4WHO: http://www.who.int/mediacentre/factsheets/fs378/en/
Background • Timing of vaccination dependent on: • Prevalence/Incidence • Ability to elicit an appropriate immune response • Risk of disease 5 • Adherence to the immunisation schedule has been found to be sub-optimal6 • Vaccines considered to have been received late if administered more than 4 weeks of due date7,8 5Prinja et al 2009; 6Luman et al, 2005; 7Sadoh and Ergie, 2009; 8Olusanya, 2000
Background • Delayed vaccine uptake for specific vaccines have been found to range between 2.7 for the first dose of the Oral Polio Vaccine to 16.5% for the 1st dose Measles vaccine in Ghana9 • Much higher proportions reported in Nigeria9 • First dose Diphtheria Pertussis Tetanus (DPT)- 13% • Third dose Hepatitis B vaccine- 63.8% • Evidence on factors contributing to delayed vaccine uptake has not been well explored in Ghana. 9 Laryea et al, 2014; 7Sado and Ergie, 2009
Background • Factors identified in studies elsewhere include 5,8, 10, 11, 12: • Cultural factors • Poor supervision of health workers • Poor programme planning and monitoring • Immunisation services offered on outreach basis • Hospital-based immunisation services • Maternal education • Hospital birth 5Prinja et al, 2005; 8Olusanya, 2010; 10Antai, 2009; 11Jani et al, 2008; 12Pandolfi et al, 2008; 13Sia et al, 2009;
Objective • Identify factors associated with delayed vaccine uptake among children accessing immunisation services in a teaching hospital in Ghana
Methods- Study design and Setting • Unmatched case control targeting children less than 5 years of age accessing immunisation services • 1 case to 2 controls • Cases- children for whom at least one vaccine in the immunisation schedule was taken more than 4 weeks after due date(s) • Controls- children who received all the due vaccines on or within 4 weeks of the scheduled date(s) • Study setting- Urban Immunisation Clinic
Methods- Data Collection • A sample size of 243 was estimated Statistical package Epi Info Version 7.1.4 • Data collection- structured questionnaire administered by trained research assistants • Consecutive cases of delayed vaccine uptake among attendants of the KATH MCH clinic identified for inclusion over a 6 month period • Controls were selected consecutively as cases were identified among children
Methods- Ethics • Written informed consent was obtained from all respondents • Voluntary participation • Non-participation had no impact on the quality of services provided • Respondents at liberty to discontinue at any given time • Ethical approval obtained from the KATH/ KNUST-SMS Committee on Human Research, Publications and Ethics (CHRPE)
Methods- Data Analysis • Data entry and analysis- Epi Info Version 7.1.4. • Univariate analysis • Bivariate analysis for selected variables • Estimation of Odds Ratios for categorical variables • Chi-squared tests for trend were estimated for ordinal variables. • Multivariate analysis- logistic regression for the statistically significant variables identified
Results • Almost all mothers (99.6%) accessed ANC during the pregnancy • The mean (SD) number of ANC sessions attendance was 6.3 (±1.55) with a range of 2 to 9 • Among mothers of cases the mean (SD) number of ANC visits was 6.0 (±1.90) and a range of 2 to 9 • Mothers of controls recorded a mean of 6.4 ANC visits (±1.33) with a range of 3 to 9
Results Place of delivery among children seen at the KATH MCH Clinic
Results • Spontaneous vaginal delivery- 69.8% overall with remainder by caesarean section. • 98 (40.3%) mothers admitted after delivery with a minimum of 24 hours spent post delivery • 21 children were admitted after delivery (16 were cases and 5 controls) • Among controls, reasons for admission were: Birth Asphyxia (3), Neonatal Jaundice (1) and Prematurity (1)
Results Reasons for admission among infants admitted post-delivery among cases
Results • 81 cases of delayed vaccination • 62 children (76.5%) received one vaccine later than 4 weeks of due date • 13 (16.1%) received 2 vaccines later than scheduled dates • 4 (4.9%) 3 vaccines later than scheduled dates • 1 (1.2%) 4vaccines later than scheduled dates • 1 (1.2%) 5 vaccines later than scheduled dates • A total of 109 vaccines were received late among the 81 cases • The third dose of the pentavalent vaccine (PENTA 3) was the most common vaccine received late
Results Vaccines received >4 weeks of due date
Limitations • Single clinic (teaching hospital) and generalisability • Changes in the EPI schedule for Ghana
Discussion • Hospital birth and non-receipt of recommended vaccines • Clinical indications for delaying vaccination/?? Clarity on contraindications for vaccination • PENTA 3 as a the commonest vaccine received late- implications for vaccine coverage • Maternal factors in timely vaccine administration
Conclusion • Penta 3, Measles/Yellow Fever and BCG are the commonest vaccines received late • Some children born in hospitals do not receive the recommended first vaccines • Maternal educational attainment and baby’s condition after delivery- strong predictors of vaccine timeliness
Recommendations • Targeted health education campaigns for at-risk mothers • Follow-up of defaulters to ensure adherence to schedule • Institution of intra-facility ‘outreach services’ • Inclusion of vaccination in the planned management after delivery
Recommendations- Further studies • Underlying factors for delayed vaccination among infants admitted after delivery • Explore maternal perception of risks associated with infant vaccination
List of References 1. Coffield AB, Maciosek MV, McGinns JM, Harris JR, Caldwell MB, Teutsch SM, et al. Priorities among clinical preventive services. Am J Prev Med. 2001;21(1):1–9. 2. Miller M, Hinman A. Economic Analyses of Vaccine Policies. In: Plotkin S, Orenstein W, editors. Vaccines. 4th ed. Elsevier Inc; 2004. 3. Wolfson L, Gasse F, Lee-Martin S-P, Lyndon P. Estimating the costs of achieving the WHO–UNICEF Global Immunization Vision and Strategy, 2006–2015. Bull World Health Organ. 2008;86:27–39. 4. World Health Organisation. WHO | Immunization coverage [Internet]. WHO. [cited 2016 Sep 8]. Available from: http://www.who.int/mediacentre/factsheets/fs378/en/ 5. Prinja S, Gupta M, Singha A, Kumara R. Effectiveness of planning and management interventions for improving age-appropriate immunization in rural India. Bull World Health Organ. 2009;88:97–103. 6. Luman E, Barker L, McCauley M, Drews-Botch C. Timeliness of Childhood Immunisations: A State-Specific Analysis. Am J Public Health. 2005;95(8):1367–74. 7. Sadoh A, Eregie C. Timeliness and Completion Rate of Immunization among Nigerian Children Attending a Clinic-based Immunization Service. J health populnutr. 2009; 8. Olusanya B. Patterns and Determinants of BCG immunisation Delays in Sub-Saharan African Community. Health Res Policy Syst. 2010;8:1. 9. Laryea DO, AbbeyquayeParbie E, Frimpong E. Timeliness of childhood vaccine uptake among children attending a tertiary health service facility-based immunisation clinic in Ghana. BMC Public Health. 2014 Jan 29;14:90. 10. Antai D. Inequitable childhood immunization uptake in Nigeria: a multilevel analysis of individual and contextual determinants. BMC Infectious Diseases. 2009;9:181. 11. Jani J, De Schacht C, Jani V, Bjunne G. Risk factors for Incomplete Vaccination and Missed Opportunity for Immunisation in Rural Mozambique. BMC Public Health. 2008;8:161. 12. Pandolfi E, Graziani C, Ieraci R, Cavagni G, Tozzi A. A comparison of populations vaccinated in a public service and in a private hospital setting in the same area. Biomed Cent Public Health. 2008;8(278):1–8. 13. Sia D, Pierre Fournier P, Kobiané J, Sondo B. Rates of coverage and determinants of complete vaccination of children in rural areas of Burkina Faso (1998-2003). Biomed Cent Public Health. 2009;9(416):1–10.