Download
1 / 82
890 likes | 1.17k Vues
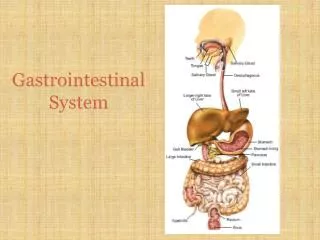
Neonatal Gastrointestinal System. Carmelita Rivero, RNC Madigan Army Medical Center. Embryology. Weeks 3,4 – Esophagus, liver, stomach, and intestine are distinct elements. Week 7 – Intestinal loops herniate into the umbilical cord.

E N D
Neonatal Gastrointestinal System Carmelita Rivero, RNC Madigan Army Medical Center
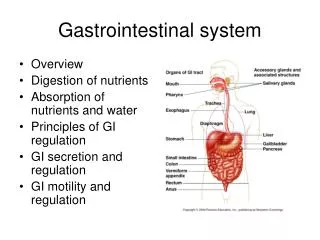
Embryology • Weeks 3,4 – Esophagus, liver, stomach, and intestine are distinct elements. • Week 7 – Intestinal loops herniate into the umbilical cord. • Week 9,10 – Intestines re-enter abdominal cavity. Intestines continue to rotate.
Embryology, cont… • Week 16 – Meconium appears and swallowing is observed. • Week 26 – Random peristalsis begins. • Week 34 – Suck/swallow become coordinated. • Week 36/38 – The GI system is mature.
Assessment • Size and Shape • normal - slightly rounded, soft, and symmetric • abnormal - • distended - intestinal obstruction, infection • scaphoid - diaphragmatic hernia • asymmetric - mass, organomegaly, intestinal obstruction
Assessment • Hernias • umbilical - common in African-American, Down’s, hypothyroid. • inguinal - more common in males • femoral - more common in females • Muscular Development • abnormal - prune-belly syndrome, diastasis recti
Assessment • Umbilicus - abnormal • green/dark yellow staining - in utero meconium passage • wet, foul smelling, or red - infection • persistent, clear, drainage - patent urachus • Thick, gelatinous - LGA • Thin, small - IUGR • 2 vessel cord - possible congenital anomalies
Assessment • Bowel sounds • Audible within 15-30 minutes after birth • Hyper/hypoactive is not necessarily pathologic. • Hyperactive - malrotation, Hirschprungs, diarrhea • Hypoactive - ileus • Palpation • Masses • Organ Enlargement - liver 1-2 cm below right costal margin, mid clavicular line.
Risk Factors • GI disease in family • Genetic syndromes • Fetal ultrasound - view of dilation or obstruction • Maternal polyhydramnios • Failure to pass meconium within 24-48 hours • Abdominal distention • Bilious vomiting
How does it happen? • Normal develop-ment fails to continue
General Treatment of GI Patients • NPO – bowel rest • IV Fluids • Gastric suction on low • Antibiotics • Surgical correction
The Esophagus Tracheoesophageal Fistula (TEF) • Incidence : 1 in 4000 live births • 50-70% of affected infants have associated anomalies.
4 Types of TE Fistulas • The most common type is the esophageal atresia with tracheoesophageal fistula (85%)
TE Fistula - Presentation • Dependent upon type of anomaly • History of polyhydramnios • Inability to swallow saliva leads to drooling • Gavage tube cannot be passed • Coughing, choking or cyanosis with feedings • Abdominal distention • Recurrent pneumonia
TE Fistula - Treatment • Elevate the head 30-45 degrees • Low suction to remove secretions from the esophageal pouch • Comfort measures • Assess for associated anomalies • Cardiac defects – 30% • GI anomalies – 12% • VATER/VACTERL – 15%
Gastroesophageal Reflux • GER - an effortless retrograde movement of gastric contents into the esophagus. • Regurgitation - movement of gastric contents into the mouth. • Physiologic reflux is a normal occurrence in infants, children, and adults. • Physiologic reflux can become a pathologic problem at any point.
Gastroesophageal Reflux • Infants with GER usually become symptomatic at 2-4 months of age, with a peak in symptoms seen at 4-5 months of age. Most resolve by 8-12 months. • This is probably due to the maturation of the GI system and the increase consumption of solid foods.
Gastroesophageal Reflux • Can result in: • Failure to thrive • Aspiration • Anemia • Esophagitis • Apnea • Reflex bronchospasm • SIDS-like events
GE Reflux : Symptoms • Fussiness • Irritability • “Colic” • Failure to thrive • Excessive regurgitation/vomiting • Refusal of feeding • Back arching with feeding • Gagging • Excess swallowing (about 30-60 minutes after feeding)
GE Reflux : Symptoms • Fussiness is probably due to pain from exposure of the esophagus to acidic gastric contents. • Infants with reflux may first present with choking, gagging, apnea, wheezing, or recurrent pneumonia. • Infant apnea often occurs 1-2 hours after feeding. • Increased work of breathing can increase abdominal pressure, pushing gastric contents back up into the espohagus
GE Reflux : Physiology • Anatomic and functional immaturity of the GI tract – Term Infants • Immaturity of the lower esophageal sphincter (LES) • Positioning of the LES • Alterations in gastric and esophageal motility • Delayed gastric emptying • air swallowing • Frequent prone positioning
GE Reflux : Treatment • Treatment for simple regurgitation • Frequent burping • Feeding slowly in a semi-upright position • Small frequent feedings • Conservative treatment for GE Reflux • Avoid supine position while awake • Avoid infant seats/swings that cause the infant to slouch. • Encourage an upright position such as an infant front pack. • Reduce smoke exposure
The Stomach Pyloric Stenosis: • Stenosis of the pyloric musculature. • Incidence – 1 of every 500 births • Males are affected 4:1 • First born more often affected, highest risk is the first born male of an affected mother. (hereditary component)
Pyloric Stenosis • Symptoms usually occur from 3-4th week of life up to the 5th month after birth. Symptoms: • Non-bilious, projectile vomiting • Dehydration • Visible peristaltic waves in epigastrium • Palpable pyloric “olive” • Failure to thrive
Abdominal Cavity Duodenal Atresia: • Congenital obstruction of the duodenum. The atresia usually occurs distal to the ampulla of Vater. • Incidence – 1 in every 10,000 live births • Females more commonly affected than males • 60-70% of cases have associated anomalies • Down’s Syndrome • Prematurity • Intestinal malrotation • Congenital heart disease • Anorectal anomalies • Tracheoesophageal abnormalities
Duodenal Atresia Presentation: • Bilious Vomiting (85%) • Abdominal distention • May pass meconium in the first 24 hours, then bowel movements cease. • Jaundice
Duodenal Atresia Diagnosis: • History of polyhydramnios • Prenatal diagnosis • Presence of bilious vomiting • CXR with “double bubble”
Malrotation • An assortment of intestinal anomalies of rotation and fixation. • Unknown incidence, occurs more often in males. • Associated with diaphragmatic hernia, intestinal atresia, omphalocele, and gastroschisis.
Malrotation • The intestine is subject to torsion around the superior mesenteric artery, occluding the blood supply. • The intestines may also twist on themselves (midgut volvulus) and occlude the intestinal lumen. • In both cases, ischemia and bowel necrosis then result. • Malrotation with volvulus is a surgical emergency. Goal is to release strangulation of the bowel.
Malrotation • Acute Symptoms: • Bilious vomiting • Abdominal distention and pain • Rectal bleeding • Signs of shock and sepsis • “Less Acute Cases”: • Failure to thrive • Intermittent bilious vomiting • Abdominal tenderness
Omphalocele • The herniation of abdominal viscera into the umbilical cord, usually covered by a pertoneal sac and with the umbilical arteries and veins inserting into the apex of the defect. • Believed to be caused by incomplete closure of the abdominal wall or incomplete return of the bowel into the abdominal cavity.
Omphalocele • Incidence : 1 in 5,000 to 6,000 live births. • Large defects may also include the stomach, liver, and the spleen. • A rupture of the omphalocele can occur at any time, exposing the abdominal contents to amniotic fluid. • Mortality rate is related to severity of other defects; with associated heart disease is 80%, without heart disease is only 30%.
Omphalocele • 30-50% have associated anomalies: • prematurity (30%) • cardiac defects (19-25%) • neurological anomalies • genitourinary anomalies • skeletal anomalies • chromosomal anomalies (45-55%) • malrotation/atresia of the intestines
Gastroschisis • Incidence : 1 in 30,000 to 50,000 live births. • The defect is usually smaller than an omphalocele and is usually placed to the right of the umbilicus. • Believed to be caused by failed closure of the lateral fold of the abdominal wall or an intrauterine vascular accident involving the omphalomesenteric artery with disruption of the umbilical ring causing herniation of the abdominal contents.
Gastroschisis • Gastroschisis usually includes the small and large intestines and rarely, the liver. • The intestines are thick, edematous, and inflamed d/t exposure to amniotic fluid. • 10% have intestinal malrotation and atresia,40% are either premature or SGA,but other anomalies are uncommon. • Mortality rate is 10-30%
Abdominal Wall Defects Treatment: • Cover the bowel with a sterile plastic bag. Monitor the baby’s temperature, fluid and electrolytes closely. • Position the baby on his side and support the defect. • Handle bowel as little as possible, and, If necessary, use sterile gloves.
Necrotizing Enterocolitis • An acquired disease that affects the GI system, particularly of premature infants. It is characterized by areas of necrotic bowel, both large and small intestines. • Incidence: 70-90% occur in preterm infants. • Cases occur sporadically and in clusters • Mortality rate greatly exceeds all other GI surgical disorders.
NEC - Risk Factors • Most important risk factor – prematurity
Necrotizing Enterocolitis • Unknown etiology, a possible combination of the following five mechanisms: • Mucosal injury • Inflammatory mediators • GI immaturity • Infectious pathogens • Feedings
Necrotizing Enterocolitis • Breastmilk may provide some protective ingredients, but NEC can occur in infants who have received breastmilk. • Breastmilk has IgA, macrophages, non-pathogenic bacteria, and secretory molecules w/anti-bacterial properties. • The bacteria promote the growth of bacteria that excrete lactic acid and acetic acid which inhibit the growth of many pathogenic gram neg. bacteria.