Download
1 / 35
380 likes | 420 Vues
Diabetic Autonomic Neuropathy (DAN). Introduction. Epidemi0logy. ● Is a serious & a common complication of DM . ● Frequently coexists with other peripheral neuropathies & other diabetic complications or may be isolated . ● Frequently precedes the detection of other complications .

E N D
Diabetic Autonomic Neuropathy (DAN)
Epidemi0logy ●Is a serious & a common complication of DM . ● Frequently coexists with other peripheral neuropathies & other diabetic complications or may be isolated . ● Frequently precedes the detection of other complications . ● Prevalence of DAN varies depending on : 1)whether studies have been carried out in the community , clinic , or tertiary referral center . 2)lack of standard accepted definition of DAN & different diagnostic methods . 3)age , sex , duration of DM , type of DM & glycemic control . ● The 5 year mortality rate of diabetics who showed symptoms of DAN & a disrupted HRV in cardiovascular autonomic function tests was 53% , compared to only 15% in diabetics without autonomic dysfunction .
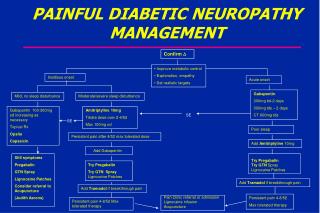
Clinical manifestations Cardiovascular :-Gastrointestinal:- Resting tachycardia Esophageal dysmotility Orthostatic hypotension Constipation Exercise intolerance Diarrhea Silent myocardial ischemia Fecal incontinence Genitourinary:-Metabolic:- Neurogenic bladder Hypoglycemic unawareness Erectile dysfunction Hypoglycemia - associated Retrograde ejaculation autonomic failure Dyspareunia Sudomotor:-Pupillary:- Anhydrosis & dry skin Decrease diameter of dark - Heat intolereance adapted pupil
Differential Diagnosis (1)Pure autonomic failure (formerly called idiopathic orthostatic hypotension) (2)Multiple system atrophy with autonomic failure (formerly called Shy - Drager syndrome) (3)Addison’s disease & hypopituitarism (4)Hypovolemia (5)Peripheral autonomic neuropathies (e.g amyloid neuropathy , idiopathic autonomic neuropathy) (6)Medications (e.g sympathetic blockers , vasodilators )
Pathophysiology Possible pathological mechanisms of diabetic neuropathy : ● Disorders of polyol metabolism ● Disorders of FA metabolism ● Accumulation of glycated proteins ● Endoneural ischemia ● Oxidative stress ● Destruction of nerve growth factors & axonal transport ● Immunological : autoimmune , inflammatory response
To study autonomic changes that accompany diabetic neuropathy
The tests were done on 2 groups : Control group (n=2) : Known healthy subjects Diabetic neuropathy group (n=2) : Known diabetic patients complicated with peripheral neuropathy
Sphygmomanometer Bridge amplifier Bio amplifier
Pneumotracer ECG leads
Disposable syringe Hand grip
Screening (A)Parasympathetic tests :- HR response to deep breathing :- - The patient breathes deeply for 3 cycles . - Greatest HR difference during each cycle is measured & the differences are averaged . Normal :≥ 15 BPM Borderline : 11-14 BPM Abnormal : ≤ 10 BPM
HR response to Valsalva :- • Subject breathes into disposable cardboard mouthpiece attached to sphygmomanometer to keep pressure at 40 mmHg for 15 sec . • Ratio of longest R-R within 20 beats of ending manouvre to shortest R-R during manouvre . • Test is done 3 times & the average ratio is measured . Normal :≥ 1.21 Abnormal : ≤ 1.20
HR response to standing :-30 : 15 ratio Longest R-R at 30th beat & Shortest R-R at 15th beat Normal :≥ 1.04 Borderline : 1.01-1.04 Abnormal : ≤ 1.00
B)Sympathetic tests :- BP response to standing :- Normal :≤ 10 mmHg Borderline : 11-20 mmHg Abnormal : ≥ 30 mmHg
BP response to sustained handgrip :- - Maintaining handgrip at 30% of max. voluntary pressure for up to 5 min . - Systolic BP is recorded every min . - Stop if rise reaches normal level . If not , record just before handgrip release at 5 min . Normal :≥ 16 mmHg Borderline : 11-15 mmHg Abnormal : ≤ 10 mmHg
► The tests described are based on the responses of HR & BP to variety of stimuli . ► The first 3 tests reflect cardiac parasympathetic integrity . While the last 2 tests start to give abnormal results with more severe sympathetic nerve damage . ► While each test may be used individually , all 5 should be performed when possible , so giving fuller information about the state of the autonomic nervous system . ► These tests are valid as specific markers of autonomic neuropathy if the following has been carefully ruled out & taken into consideration : 1-End-organ failure & other concomitant illness 2-Drug use (including anti-depressants , over-the-counter antihistaminics & cough , cold preparations , diuretics & aspirin) 3-Life style issues (such as exercise , smoking & caffeine intake) 4-Age
Grading Normal :All tests normal or 1 borderline Mildly abnormal : One of the 3 HR tests abnormal or 2 borderline Definitely abnormal : ≥ 2 of the HR tests abnormal Severely abnormal : ≥ 2 of the HR tests abnormal plus one or both of the BP tests abnormal , or both borderline EWING DJ, CLARKE BF (1982):Diagnosis and management of diabetic autonomic neuropathy. BRITISH MEDICAL JOURNAL; 285 2 OCTOBER :916-18.
► By studying the results of the control group & the diabetic neuropathy group , we found that : - HRV with deep respiration was below the normal level in patient 1 while it was normal in patient 2 . -There was no abnormality detected in results of Valsalva test & HR response to standing in both patients . -The result of BP response to sustained handgrip was below the normal level in patient 1 . -Results of BP response to standing test in patient 2 was borderline . -To conclude , patient 1 has both sympathetic & parasympathetic affection . On the other hand patient 2 is normal , yet the sympathetic system starts to be affected .
►The natural history of autonomic damage in diabetic patients is becoming clearer , with parasympathetic damage occurring earlier . Ewing DJ, Campbell IW, Clarke BF (1981): Heart rate changes in diabetes Mellitus. Lancet;i:183-6. However , this isn’t always the fact , sometimes the sympathetic system may be affected earlier than parasympathetic system . (http://care.diabetesjournals.org/content/26/5/1553.full)