Download
1 / 27
270 likes | 418 Vues
Cont. Alcoholism. Other examples:intoxication throughout the dayinability to cut down or stoprepeated efforts to controlcontinued use in spite of physiological problemneed for daily use to functionepisodes of blackoutsimpairment in social/occupational functioning, ie., failure to meet obligat

E N D
1. PSYC 2621 Substance Abuse and Dependence Psychoactive Substance Use Disorder
Alcoholism
Symptoms
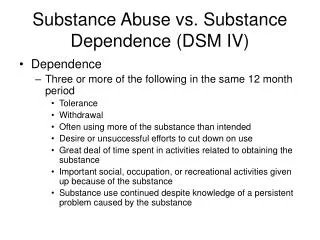
Maladaptive pattern of pathological use leading to clinically significant impairment or distress.
Failure to fulfill role obligations at work, home, or school
Using drug in hazardous situations
Recurrent arrests for drug use
Persistent conflict about use of drug
2. Cont. Alcoholism Other examples:
intoxication throughout the day
inability to cut down or stop
repeated efforts to control
continued use in spite of physiological problem
need for daily use to function
episodes of blackouts
impairment in social/occupational functioning, ie., failure to meet obligations
display erratic/impulsive behavior legal problems
inappropriate expression of aggression
3. Substance Dependence The development of physiological signs of dependence.
Lack of control over drug use
May experience tolerance or withdrawal
4. Drugs associated with dependence/abuse: Alcohol
Opiods
Stimulants (amphetamines and cocaine)
Sedatives and barbiturates
Prescription tranqulizers
Some hallucinogens
5. Facts about Addiction More men are durg and alcohol dependent than women but the gender gap is lessening at least among non-Blacks.
6. Risk Factors Low SES
Low education
unemployed
living alone
No religious preferences
7. Stages of Addiction Experimentation
Continued use of drug due to intoxicating effects
Denial
Loss of control
8. Depressants Alcohol
Leading drug of abuse
Risk factors
gender - men
age
anti-social PD
Family history
Low SES, Low education, living alone
9. Cont. Depressants: alcohol Physiological effects of Alcohol
heighten sensitivity of GABA, an inhibitory neurotransmitter, depressing the nervous system
Chronic use is associated with some forms of cancer, coronary heart disease, ulcers hypertension, gout, pancreatitis, liver diseases such as hepatitis and cirrhosis, malnutrition, Korsakoff�s Syndrome (amnesia d/o), Fetal Alcohol Syndrome (found in women who drink as little as 2 oz/day during the first trimester)
10. Cont. Depressants: alcohol Some evidence of benefits of light to moderate consumption reduces risks of heart attack.
11. Cont. Depressants Sedatives, hypnotics, and anti-anxiety drugs
Barbiturates (phenobarbital - epilepsy) are used to treat anxiety, high blood pressure.
Addicting
12. Cont. Depressants Opiods
Natural opiods: morphine, heroin, codeine derived from juice of poppy plant
Synthetic opiods: Demerol, Percodan, Darvon
pain relievers
Produce pleasurable effects because they stimulate brain centers that regulate sensations of pleasure and pain.
Endorphins: endogenous morphine
Morphine
Heroine: God�s own medicine. Withdrawal begins 4 -6 hours after last dose with flu-like symptoms; rarely die.
13. Stimulants Amphetamines
Speed
Uppers
bennies
Meth
Cocaine
Used in Coca-Cola
14. Cont. Stimulants Nicotine
400,000 died from smoking related causes
Withdrawal:
decrease energy,
nervousness
lightheadedness
headaches
insomnia
tremors
15. Hallucinogens LSD
PCP: angel-dust
Marijuana
16. Theoretical Perspectives Some adolescents use because of peer pressure or rebelling.
Biological
Normal endorphins but with opiods no endorphins so depend on drug for feeling of comfort, pleasure.
17. Cont. Theoretical Perspectives Cont. Biological
Genetic Factors
evidence to support: adoption, cross-species, but twins yield mixed results.
Identify the gene linked to dopamine receptors in brain but unknown how it contributes to alcoholism.
Research with GABA levels in sons of alcoholics showed that the sons had lower GABA (associated with anxiety/tension) than sons of nonalcoholics. When they drank, their GABA level rose to normal.
18. Cont. Theoretical Perspectives Cont. Biological
Genetic research
Sons of alcoholics tend to produce fewer alpha waves. For most people, when drink, alpha waves increase.
1/3 alcoholics show no family history. Other factors
instability in early home life
father had a low status job
availability of alcohol peer pressure
permissiveness attitude about drunkenness
19. Cont. Theoretical Learning
Drug use is a positive reinforcement
reduces tension
self-medication for depression/anxiety
With dependence comes negative reinforcement
drink to relieve the shakes, tachycardia, sweating
Classical Conditioning
the cues associated with drug use can elicit conditioned responses in the form of cravings
20. Cont. Theoretical Perspectives Cognitive
Expectancies
People choose to use or not based on expected positive or negative consequences.
According to Hull�s self-awareness model, depressants can create psychological shield to protect users from negative social feedback.
21. Cont. Theoretical Sociocultural
Culture and religion influence attitudes
Psychodynamic
Oral fixation
Dependent personality
Research is mixed
22. Treatment Biological
Detox
Disulfiram (Antabuse)
Antidepressants: stem cravings for cocaine
Nicotine replacement (long-term ineffective unless behavior modification to change habits)
Methadone (to treat withdrawal from Heroin, taken indefinitely)
Naloxone (prevents users from getting high)
23. Cont. Treatment Nonprofessional support group
Alcoholics Anonymous (AA)
90% drop out after a few meetings.
Limited controlled studies
Residential approaches
Hospitalization when need to control/provide a drug free environment, safe withdrawal, protection from suicide/homicide
Communal opportunity: Daytop/Phoenix House
24. Cont. Treatment Psychodynamic
Resolve underlying conflicts
to focus on abuse is superficial
Behavioral
change behavior when faced with temptation
Self-control strategies: ABC
A = antecedents that trigger abuse
B= behaviors
C=consequences (either reinforcing or punishing
25. Cont. Treatment Aversive conditioning
Rapid smoking
Covert sensitization (imaginal)
Social skills training
26. Cont. Treatment Relapse Prevention
50-90% will relapse
develop skills to cope with temptations/high risk situations
negative moods
interpersonal conflicts
social situations
Abstinence Violation Effect (AVE
Overreact to a lapse which leads to self-perceived weakness, shame, guilt
27. Cont. Treatment Disease model
Interpretation of lapse determines relapse
Social support is the key to relapse prevention.