Download
1 / 50
500 likes | 867 Vues
Topic 10 Brain Damage and Neuroplasticity. Can the Brain Recover from Damage?. Causes of Brain Damage. Brain tumors Cerebrovascular disorders Closed-head injuries Infections of the brain Neurotoxins Genetic factors. Brain Tumors.

E N D
Topic 10 Brain Damage and Neuroplasticity Can the Brain Recover from Damage?
Causes of Brain Damage • Brain tumors • Cerebrovascular disorders • Closed-head injuries • Infections of the brain • Neurotoxins • Genetic factors
Brain Tumors • A tumor (neoplasm) is a mass of cells that grows independently of the rest of the body – a cancer • ~20% of brain tumors are meningiomas – encased in meninges • Encapsulated, growing within their own membranes • Usually benign, surgically removable
Brain Tumors • Most brain tumors are infiltrating • Grow diffusely through surrounding tissue • Malignant, difficult to remove or destroy • About 10% of brain tumors are metastatic – they originate elsewhere, usually the lungs
Cerebrovascular Disorders • Stroke – a sudden-onset cerebrovascular event that causes brain damage • Cerebral hemorrhage – bleeding in the brain • Cerebral ischemia – disruption of blood supply • 3rd leading cause of death in the US and most common cause of adult disability
Cerebrovascular Disorders • Cerebral hemorrhage – blood vessel ruptures • Aneurysm – a weakened point in a blood vessel that makes a stroke more likely. May be congenital or due to poison or infection. • Congenital – present at birth • Cerebral ischemia – disruption of blood supply • Thrombosis – plug forms • Embolism – plug forms elsewhere and moves to the brain • Arteriosclerosis – wall of blood vessels thicken, usually due to fat deposits
Damage due to Cerebral Ischemia • Does not develop immediately • Most damage is a consequence of excess neurotransmitter release – especially glutamate • Blood-deprived neurons become overactive and release glutamate • Glutamate overactivates its receptors, especially NMDA receptors leading to an influx of Na+ and Ca++
Damage due to Cerebral Ischemia • lnflux of Na+ and Ca++ triggers: • the release of still more glutamate • a sequence of internal reactions that ultimately kill the neuron • Ischemia-induced brain damage • takes time • does not occur equally in all parts of the brain • mechanisms of damage vary with the brain structure affected
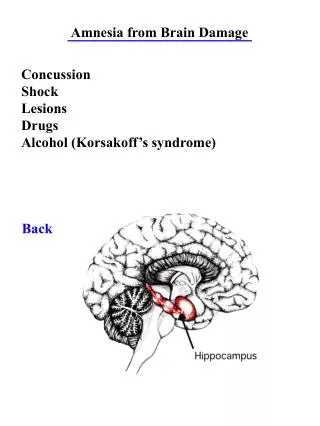
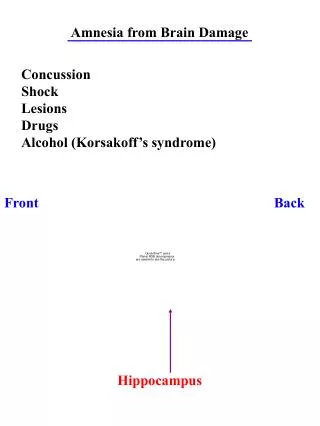
Closed-Head Injuries • Brain injuries due to blows that do not penetrate the skull – the brain collides with the skull • Contrecoup injuries – contusions are often on the side of the brain opposite to the blow • Contusions – closed-head injuries that involve damage to the cerebral circulatory system. A hematoma, a bruise, forms. • Concussion – when there is a disturbance of consciousness following a blow to the head and no evidence of structural damage.
Concussions • While there is no apparent brain damage with a single concussion, multiple concussions may result in a dementia referred to as “punch-drunk syndrome” • When might this occur? • Can it be prevented?
Brain Infection • Invasion of the brain by microorganisms • Encephalitis – the resulting inflammation • Bacterial infections • Often leads to abscesses, pockets of pus • May inflame meninges, creating meningitis • Treat with penicillin and other antibiotics • Viral infections • Some viral infections preferentially attack neural tissues
Brain Infections - Some Causes • Bacterial • Syphilis – may produce a syndrome of insanity and dementia known as general paresis • Syphilis bacteria are passed to the noninfected and enter a dormant stage for many years. • Viral • Rabies – high affinity for the nervous system • Mumps and herpes – typically attack tissues other than the brain • Viruses may lie dormant for years
Neurotoxins • May enter general circulation from the GI tract, lungs, or through the skin • Toxic psychosis – chronic insanity produced by a neurotoxin. • The Mad Hatter – may have had toxic psychosis due to mercury exposure
Neurotoxins • Some antipyschotic drugs produce a motor disorder caused tardive dyskinesia • Recreational drugs, such as alcohol, may cause brain damage • Neurotoxic effects of alcohol • Thiamine deficiency • Some neurotoxins are endogenous – produced by the body
Genetic Factors • Most neuropsychological diseases of genetic origin are associated with recessive genes. Why? • Down syndrome • 0.15% of births, probability increases with advancing maternal age • Extra chromosome 21 • Characteristic disfigurement, mental retardation, other health problems
Autistic Disorder • A chronic disorder whose symptoms include failure to develop normal social relations with other people, impaired development of communicative ability, lack of imaginative ability, and repetitive, stereotypical movements.
Possible causes • Biological • Autism was once believed to beacquired through interactions with hostile, withdrawn parents. • Research and mental health professionals are convinced autism is caused by biological factors. • Between 2 and 3 percent of siblings of people with autism are themselves autistic. • There is a 70 percent concordance rate for monozygotic twins.
Possible causes • Phenylketonuria (PKU) • A hereditary disorder caused by the absence of an enzyme that converts the amino acid phenylalanine to tyrosine; causes brain damage unless a special diet is implemented soon after birth. • Brain pathology • Heritable aspect of autism suggests the disorder is a result of structural or biochemical abnormalities in the brain. • Researchers have found evidence for structural abnormalities in the brains of autistics, but so far we cannot point to any single abnormality as the cause of the disorder.
Attention-Deficit/Hyperactivity Disorder • A disorder characterized by uninhibited responses, lack of sustained attention, and hyperactivity; first shows itself in childhood. • ADHD is the most common behavior disorder that shows itself in childhood. • ADHD is seen in 4 to 5% of grade school children.
Possible causes • Genetics • There is strong evidence from family and twin studies for hereditary factors in a person’s likelihood of developing ADHD. • Learning • Some evidence suggests impulsive and hyperactive behaviors are a result of a steep delay of reinforcement gradient.
Possible causes • Biological • There is evidence to suggest that abnormalities in dopaminergic transmission play a role in ADHD. • Brain structures • Studies of brain structure of people with ADHD do not reveal any localized abnormalities, though the total volume of their brains is approximately 4% smaller than normal.
Epilepsy • Primary symptom is seizures, but not all who have seizures have epilepsy • Epileptics have seizures generated by their own brain dysfunction • Affects about 1% of the population • Difficult to diagnose due to the diversity and complexity of epileptic seizures
Epilepsy • Types of seizures • Convulsions – motor seizures • Some are merely subtle changes of thought, mood, or behavior • Causes • Brain damage • Genes – over 70 known so far • Diagnosis • EEG – Electroencephalogram • Seizures associated with high amplitude spikes
Epilepsy • Seizures often preceded by an aura, such as a smell, hallucination, or feeling • Aura’s nature suggests the epileptic focus • Warns epileptic of an impending seizure • Partial epilepsy – does not involve the whole brain • Generalized epilepsy – involve the entire brain
Partial Seizures • Simple • symptoms are primarily sensory or motor or both (Jacksonian seizures) • symptoms spread as epileptic discharge spreads • Complex – often restricted to the temporal lobes (temporal lobe epilepsy) • patient engages in compulsive and repetitive simple behaviors – automatisms • more complex behaviors seem normal
Generalized Seizures • Grand mal • Loss of consciousness and equilibrium • Tonic-clonic convulsions • -rigidity (tonus) and tremors (clonus) • Resulting hypoxia may cause brain damage • Petit mal • not associated with convulsions • A disruption of consciousness associated with a cessation of ongoing behavior
Parkinson’s Disease • A movement disorder of middle and old age affecting ~ .5%of the population • Pain and depression commonly seen before the full disorder develops • Tremor at rest is the most common symptom of the full-blown disorder • Dementia is not typically seen • No single cause
Parkinson’s Disease • Associated with degeneration of the substantia nigra whose neurons use dopamine • Almost no dopamine in the substantia nigra of Parkinson’s patients • Treated temporarily with L-dopa • Linked to ~10 different gene mutations
Huntington’s Disease • Also a progressive motor disorder of middle and old age – but rare, with a strong genetic basis, and associated with dementia. • Begins with fidgetiness and progresses to jerky movements of entire limbs and sever dementia • Death usually occurs within 15 years • Caused by a single dominant gene • 1st symptoms usually not seen until age 40
Multiple Sclerosis • A progressive disease that attacks CNS myelin, leaving areas of hard scar tissue (sclerosis) • Nature and severity of deficits vary with the nature, size, and position of sclerotic lesions • Periods of remission are common • Symptoms include visual disturbances, muscle weakness, numbness, tremor, and loss of motor coordination (ataxia)
Multiple Sclerosis • Epidemiological studies find that incidence of MS is increased in those who spend childhood in a cool climate • MS is rare amongst Africans and Asians • Strong genetic predisposition and many genes involved • An autoimmune disorder – immune system attacks myelin • Drugs may retard progression or block some symptoms
Alzheimer’s Disease • Most common cause of dementia – likelihood of developing it increases with age • Progressive, with early stages characterized by confusion and a selective decline in memory • Definitive diagnosis only at autopsy – must observe neurofibrillary tangles and amyloid plaques
Neuropsychological Diseases - Recap • Epilepsy – abnormal electrical activity • Parkinson’s disease • progressive motor disorder without dementia • Huntington’s disease • progressive motor disorder with dementia • Multiple sclerosis • autoimmune disorder that affects motor function and strikes early • Alzheimer’s disease - dementia
Animal Models of Human Neuropsychological Diseases • While animal models only model some aspects of the human condition, they can provide insight • Kindling model of epilepsy • Experimentally induced seizure activity • Transgenic mouse model of Alzheimer’s • Mice producing human amyloid • MPTP model of Parkinson’s • Drug-induced damage comparable to that seen in PD
Kindling Model of Epilepsy • A series of periodic brain stimulations eventually elicits convulsions – the kindling phenomenon • Neural changes are permanent • Produced by stimulation distributed over time • Convulsions are similar to those seen in some forms of human epilepsy – but they only occur spontaneously if kindled for a very long time • Kindling phenomenon is comparable to the development of epilepsy (epileptogenesis) seen following a head injury
MPTP Model of Parkinson’s Disease • The Case of the Frozen Addicts • Synthetic heroin produced the symptoms of Parkinson’s • Contained MPTP • MPTP causes cell loss in the substantia nigra, like that seen in PD • Animal studies led to the finding that deprenyl can retard the progression of PD
Neuroplastic Responses to Nervous System Damage • Degeneration - deterioration • Regeneration – regrowth of damaged neurons • Reorganization • Recovery
Degeneration • Cutting axons is a common way to study responses to neuronal damage • Anterograde - degeneration of the distal segment – between the cut and synaptic terminal • cut off from cell’s metabolic center • swells and breaks off within a few days • Retrograde – degeneration of the proximal segment – between the cut and cell body • progresses slowly • if regenerating axon makes a new synaptic contact, the neuron may survive
Neural Regeneration • Does not proceed successfully in mammals and other higher vertebrates - capacity for accurate axonal growth is lost in maturity • Regeneration is virtually nonexistent in the CNS of adult mammals and unlikely, but possible, in the PNS
Neural Regeneration in the PNS • If the original Schwann cell myelin sheath is intact, regenerating axons may grow through them to their original targets • If the nerve is severed and the ends are separated, they may grow into incorrect sheaths • If ends are widely separated, no meaningful regeneration will occur
Neural Reorganization • Reorganization of 1° sensory and motor systems has been observed following damage to: • peripheral nerves • primary cortical areas • Lesion one retina and remove the other – V1 neurons that originally responded to lesioned area now responded to an adjacent area – remapping occurred within minutes • Studies show scale of reorganization possible is far greater than anyone assumed possible
How/why does damage lead to reorganization? • Strengthened existing connections due to a release from inhibition? • Consistent with speed and localized nature of reorganization • Establishment of new connections? • Magnitude can be too great to be explained by changes in existing connections
Recovery of Function after Brain Damage • Difficult to conduct controlled experiments on populations of brain-damaged patients • Can’t distinguish between true recovery and compensatory changes • Cognitive reserve – education and intelligence – thought to play an important role in recovery of function – may permit cognitive tasks to be accomplished new ways • Adult neurogenesis may play a role in recovery
Treating Nervous System Damage • Reducing brain damage by blocking neurodegeneration • Promoting recovery by promoting regeneration • Promoting recovery by transplantation • Promoting recovery by rehabilitative training
Reducing brain damage by blocking neurodegeneration • Various neurochemicals can block or limit neurodegeneration • Apoptosis inhibitor protein – introduced in rats via a virus • Nerve growth factor – blocks degeneration of damaged neurons • Estrogens – limit or delay neuron death • Neuroprotective molecules tend to also promote regeneration
Promoting Recovery by Promoting Regeneration • While regeneration does not normally occur in the CNS, experimentally it can be induced • Eliminate inhibition of oligodendroglia and regeneration can occur • Provide Schwann cells to direct growth
Promoting Recovery by Neurotransplantation • Fetal tissue • Fetal substantia nigra cells used to treat MPTP-treated monkeys (PD model) • Treatment was successful • Limited success with humans • Stem cells • Rats with spinal damage “cured”, but much more research is needed
Promoting Recovery by Rehabilitative Training • Constraint-induced therapy – down functioning limb while training the impaired one – create a competitive situation to foster recovery • Facilitated walking as an approach to treating spinal injury
Can the brain recover from brain damage? • Consider what you now know about the brain’s ability to adapt following brain damage, can it “recover”? • If so, what conditions promote recovery?