Download
1 / 1
10 likes | 99 Vues
10. 11. 12. Step 4 - Study of the mechanisms linking alterations of the ecological niche to the pathogenesis of the disease.

E N D
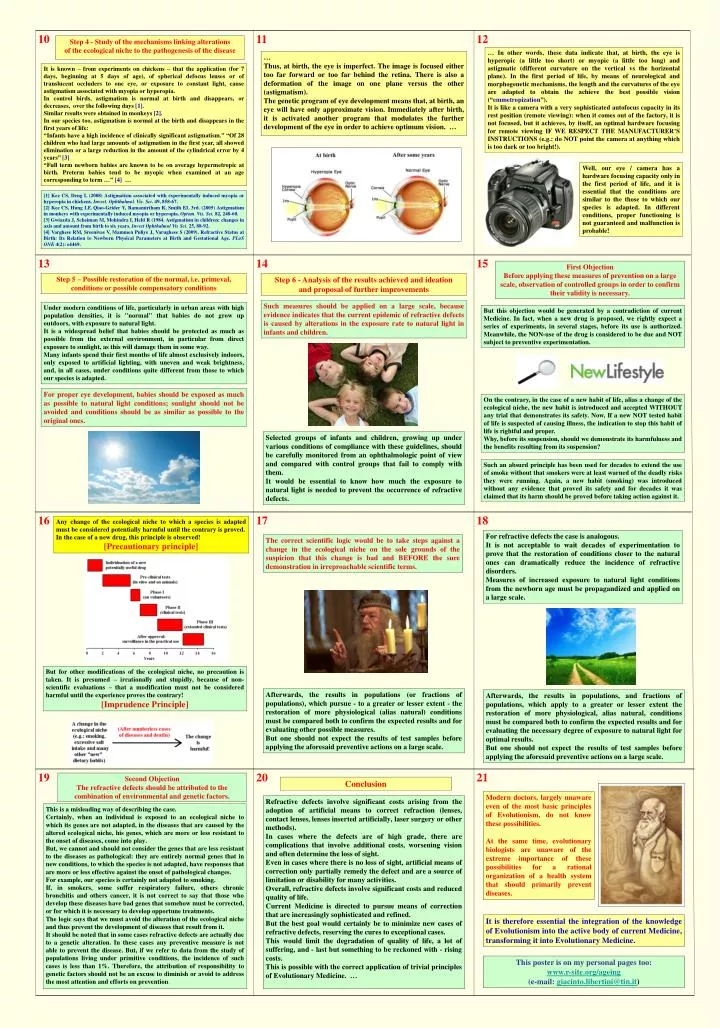
10 11 12 Step 4 - Study of the mechanisms linking alterations of the ecological niche to the pathogenesis of the disease … In other words, these data indicatethat, at birth, the eye is hyperopic (a little too short) or myopic (a little too long) and astigmatic (different curvature on the vertical vs the horizontal plane). In the first period of life, by means of neurological and morphogenetic mechanisms, the length and the curvatures of the eye are adapted to obtain the achieve the best possible vision (“emmetropization”). It is like a camera with a very sophisticated autofocus capacity in its rest position (remote viewing): when it comes out of the factory, it is not focused, but it achieves, by itself, an optimal hardware focusing for remote viewing IF WE RESPECT THE MANUFACTURER’S INSTRUCTIONS (e.g.: do NOT point the camera at anything which is too dark or too bright!). … Thus, at birth, the eye is imperfect. The image is focused either too far forward or too far behind the retina. There is also a deformation of the image on one plane versus the other (astigmatism). The genetic program of eye development means that, at birth, an eye will have only approximate vision. Immediately after birth, it is activated another program that modulates the further development of the eye in order to achieve optimum vision. … It is known – from experiments on chickens – that the application (for 7 days, beginning at 5 days of age), of spherical defocus lenses or of translucent occluders to one eye, or exposure to constant light, cause astigmatism associated with myopia or hyperopia. In control birds, astigmatism is normal at birth and disappears, or decreases, over the following days [1]. Similar results were obtained in monkeys [2]. In our species too, astigmatism is normal at the birth and disappears in the first years of life: “Infants have a high incidence of clinically significant astigmatism.” “Of 28 children who had large amounts of astigmatism in the first year, all showed elimination or a large reduction in the amount of the cylindrical error by 4 years” [3] “Full term newborn babies are known to be on average hypermetropic at birth. Preterm babies tend to be myopic when examined at an age corresponding to term …” [4] … Well, our eye / camera has a hardware focusing capacity only in the first period of life, and it is essential that the conditions are similar to the those to which our species is adapted. In different conditions, proper functioning is not guaranteed and malfunction is probable! [1] Kee CS, Deng L (2008) Astigmatism associated with experimentally induced myopia or hyperopia in chickens. Invest. Ophthalmol. Vis. Sci. 49, 858-67. [2] Kee CS, Hung LF, Qiao-Grider Y, Ramamirtham R, Smith EL 3rd. (2005) Astigmatism in monkeys with experimentally induced myopia or hyperopia. Optom. Vis. Sci. 82, 248-60. [3] Gwiazda J, Scheiman M, Mohindra I, Held R (1984. Astigmatism in children: changes in axis and amount from birth to six years. Invest Ophthalmol Vis Sci. 25, 88-92. [4] Varghese RM, Sreenivas V, Mammen Puliye J, Varughese S (2009). Refractive Status at Birth: Its Relation to Newborn Physical Parameters at Birth and Gestational Age. PLoS ONE 4(2): e4469. 13 14 15 First Objection Before applying these measures of prevention on a large scale, observation of controlled groups in order to confirm their validity is necessary. Step 5 – Possible restoration of the normal, i.e. primeval, conditions or possible compensatory conditions Step 6 - Analysis of the results achieved and ideation and proposal of further improvements Such measures should be applied on a large scale, because evidence indicates that the current epidemic of refractive defects is caused by alterations in the exposure rate to natural light in infants and children. Under modern conditions of life, particularly in urban areas with high population densities, it is "normal" that babies do not grow up outdoors, with exposure to natural light. It is a widespread belief that babies should be protected as much as possible from the external environment, in particular from direct exposure to sunlight, as this will damage them in some way. Many infants spend their first months of life almost exclusively indoors, only exposed to artificial lighting, with uneven and weak brightness, and, in all cases, under conditions quite different from those to which our species is adapted. But this objection would be generated by a contradiction of current Medicine. In fact, when a new drug is proposed, we rightly expect a series of experiments, in several stages, before its use is authorized. Meanwhile, the NON-use of the drug is considered to be due and NOT subject to preventive experimentation. For proper eye development, babies should be exposed as much as possible to natural light conditions; sunlight should not be avoided and conditions should be as similar as possible to the original ones. On the contrary, in the case of a new habit of life, alias a change of the ecological niche, the new habit is introduced and accepted WITHOUT any trial that demonstrates its safety. Now, If a new NOT tested habit of life is suspected of causing illness, the indication to stop this habit of life is rightful and proper. Why, before its suspension, should we demonstrate its harmfulness and the benefits resulting from its suspension? Selected groups of infants and children, growing up under various conditions of compliance with these guidelines, should be carefully monitored from an ophthalmologic point of view and compared with control groups that fail to comply with them. It would be essential to know how much the exposure to natural light is needed to prevent the occurrence of refractive defects. Such an absurd principle has been used for decades to extend the use of smoke without that smokers were at least warned of the deadly risks they were running. Again, a new habit (smoking) was introduced without any evidence that proved its safety and for decades it was claimed that its harm should be proved before taking action against it. 16 17 18 Any change of the ecological niche to which a species is adapted must be considered potentially harmful until the contrary is proved. In the case of a new drug, this principle is observed! [Precautionary principle] For refractive defects the case is analogous. It is not acceptable to wait decades of experimentation to prove that the restoration of conditions closer to the natural ones can dramatically reduce the incidence of refractive disorders. Measures of increased exposure to natural light conditions from the newborn age must be propagandized and applied on a large scale. The correct scientific logic would be to take steps against a change in the ecological niche on the sole grounds of the suspicion that this change is bad and BEFORE the sure demonstration in irreproachable scientific terms. But for other modifications of the ecological niche, no precaution is taken. It is presumed – irrationally and stupidly, because of non-scientific evaluations – that a modification must not be considered harmful until the experience proves the contrary! [Imprudence Principle] Afterwards, the results in populations (or fractions of populations), which pursue - to a greater or lesser extent - the restoration of more physiological (alias natural) conditions must be compared both to confirm the expected results and for evaluating other possible measures. But one should not expect the results of test samples before applying the aforesaid preventive actions on a large scale. Afterwards, the results in populations, and fractions of populations, which apply to a greater or lesser extent the restoration of more physiological, alias natural, conditions must be compared both to confirm the expected results and for evaluating the necessary degree of exposure to natural light for optimal results. But one should not expect the results of test samples before applying the aforesaid preventive actions on a large scale. 19 20 21 Second Objection The refractive defects should be attributed to the combination of environmental and genetic factors. Conclusion Modern doctors, largely unaware even of the most basic principles of Evolutionism, do not know these possibilities. At the same time, evolutionary biologists are unaware of the extreme importance of these possibilities for a rational organization of a health system that should primarily prevent diseases. Refractive defects involve significant costs arising from the adoption of artificial means to correct refraction (lenses, contact lenses, lenses inserted artificially, laser surgery or other methods). In cases where the defects are of high grade, there are complications that involve additional costs, worsening vision and often determine the loss of sight. Even in cases where there is no loss of sight, artificial means of correction only partially remedy the defect and are a source of limitation or disability for many activities. Overall, refractive defects involve significant costs and reduced quality of life. Current Medicine is directed to pursue means of correction that are increasingly sophisticated and refined. But the best goal would certainly be to minimize new cases of refractive defects, reserving the cures to exceptional cases. This would limit the degradation of quality of life, a lot of suffering, and - last but something to be reckoned with - rising costs. This is possible with the correct application of trivial principles of Evolutionary Medicine. … This is a misleading way of describing the case. Certainly, when an individual is exposed to an ecological niche to which its genes are not adapted, in the diseases that are caused by the altered ecological niche, his genes, which are more or less resistant to the onset of diseases, come into play. But, we cannot and should not consider the genes that are less resistant to the diseases as pathological: they are entirely normal genes that in new conditions, to which the species is not adapted, have responses that are more or less effective against the onset of pathological changes. For example, our species is certainly not adapted to smoking. If, in smokers, some suffer respiratory failure, others chronic bronchitis and others cancer, it is not correct to say that those who develop these diseases have bad genes that somehow must be corrected, or for which it is necessary to develop opportune treatments. The logic says that we must avoid the alteration of the ecological niche and thus prevent the development of diseases that result from it. It should be noted that in some cases refractive defects are actually due to a genetic alteration. In these cases any preventive measure is not able to prevent the disease. But, if we refer to data from the study of populations living under primitive conditions, the incidence of such cases is less than 1%. Therefore, the attribution of responsibility to genetic factors should not be an excuse to diminish or avoid to address the most attention and efforts on prevention. It is therefore essential the integration of the knowledge of Evolutionism into the active body of current Medicine, transforming it into Evolutionary Medicine. This poster is on my personal pages too: www.r-site.org/ageing (e-mail: giacinto.libertini@tin.it)