Download
1 / 87
3.11k likes | 11.72k Vues
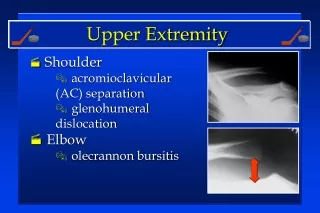
Shoulder Dislocation. By: Hashem Bukhary. ANATOMY The most commonly dislocated joint in the body, Why ? S tability is sacrificed for High Motion Small (ball & Socket Joint). Muscle That contribute to shoulder joint. Glenoid Tubricle is “ Log.H Biceps Attachment ”.

E N D
Shoulder Dislocation By: Hashem Bukhary
ANATOMY The most commonly dislocated joint in the body, Why ? Stability is sacrificed for High Motion Small (ball & Socket Joint)
Types: Anterior ( 90-95 % ) Posterior ( 2-5 % ) Inferior (<1%)
Shared Complication • Recurrence “ Most Common “ (Esp: <30) • Nerve Injury (Esp: Axillary) • Rotator cuff or capsular tear ( Esp : Old )
Recurrence Recurrence rate depends on age of 1st dislocation: <20 yrs = 65-95%; 20-40 yrs = 60-70%; >40 yrs = 4-20%
Nerve Injury Axillary N. “Post. Crod” = Teris Minor and deltoid Mus. + skin over Shoulder Numbness & Weakness “ Transient Nuropraxia” “ 5%” Musculocutaneous nerve (sensory patch on lateral forearm)
The "regimental badge" area Examine pin-prick sensation to this area to assess axillary nerve sensory function.
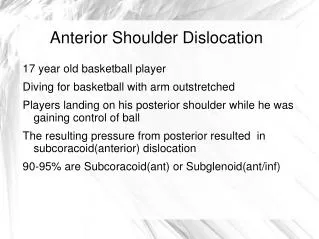
Anterior Dislocation Subcoracoid(90%), Subglenoid(7%), Subclavicular(<3%)
Anterior Dislocation 1/ Hx and Mechanism : Traumatic VS Atraumatic Posteriordirect force OR Blow to Posteriorshoulder : with position [ Abduction + Extension + Ext. Rot ] VS Loose joint with more stretching [ Chronic pain or feeling of instability ]
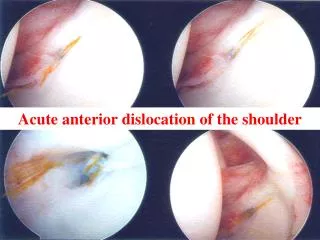
Anterior Dislocation 1/ Hx, Ex and Mechanism : Sever Pain. Lat. outline shoulder flattened. Possible bulge under acromion. Possible Nerve / Vessel injury.
Anterior Dislocation 1/ Hx. Ex and Mechanism : Ass. With: (Anterio-Inferior) Labral tear [+/- Bony] = Bankart Lesion # Greater Tuberosity ( esp: > 50 yrs ) # ( Back indentation ) to Humeral “Post-Superior” Head = Hill-Sachs lesion.
Anterior Dislocation Labral tear only vs With Bony Lesion
Anterior Dislocation Post-Superior Hum. Head
Anterior Dislocation 2/ Special Ex: Apprehension Test ( In Supine/ abduct 90” & Ext. Rot)
Anterior Dislocation 2/ Special Ex: Apprehension Test ( In Supine/ abduct 90” & Ext. Rot) Relocate test ( apply Post-Pushing Force )
Anterior Dislocation 2/ Ex:
Anterior Dislocation 2/ Special Ex: Apprehension Test ( In Supine/ abduct 90” & Ext. Rot) Relocate test ( apply Post-Pushing Force ) Load & Shift test.( Humeral Head draft force ) Role OUT dislocation if pt. can Touch the opposite shoulder.
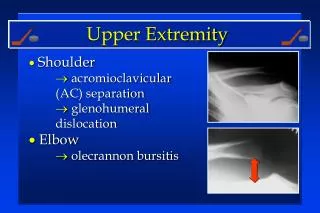
Anterior Dislocation 3/ Radiology Finding: X ray Views = AP, Trans-scapular ” Y ”, Axillary. MRI = to evaluate Labral Tear CT = for small bony #
Anterior Dislocation Lateral Scapular View
Anterior Dislocation Lateral Scapular View
Anterior Dislocation Lateral “Y”
Anterior Dislocation Axillary
Anterior Dislocation Bankart BONY Lesion
Anterior Dislocation MRI w/ Intra Articular Contrast: Anterior Labral injury
Anterior Dislocation Hill-Sach injury
Anterior Dislocation Management: Non Operative VS Operative
Anterior Dislocation Management : Non Operative (Conservative) 1/ Closed reduction with: “ IV sedation and muscle relaxation Or Local Anasthesia [ 20cc + 1% Lidocan] just below to acromion process . 2/ Imoblization 1-3 wks: Avoid abduction (still Controversial for duration & position). 3/ PT for restoring Painless ROM.
Anterior Dislocation Methods : I: Traction-countertraction: In Adduction – Seen in Hippocrates & Strap Methods. In F.F. – Seen in Stimson and Spaso In lateral elevation – Seen in the Eskimos
Hippocratic method: • Place heel into patient's axilla and apply traction to arm foot acts as a a lever to • PUSH the humeral head laterally. • 30-40° abduction • for 1 mint. Anterior Dislocation
Better to flex the Elbow 90° to relax the biceps muscle. • Most effective for Subglenoid dis. • Brach. Plex and vessel injuries are common No longer use nowadays. Anterior Dislocation
Anterior Dislocation Strap Method: With elbow 90° Assistant stabilizes body with a folded sheet wrapped across the chest while the surgeon applies gentle steady traction along the axis of the arm in 30-40° abduction.
Anterior Dislocation Strap Method: Simple, safe, effective, quick, and may be less painful. However, they require adequate space and at least two persons. Towels or sheets can cause friction injury to the fragile skin of the elderly.
Stimson (Hanging Arm) : • Pt. lies prone with arm hanging over table edge. • Hangabout 5-7 kg weight on wrist for 20-30 min . • Never let pt. Grap the wit due to engagement Long. Head of Biceps. Anterior Dislocation Management:
Stimson (Hanging Arm) : • If Still not occur spontaneously • Gentle longitudinal traction (with elbow at 90°) and internal or external rotation are applied to the arm or direct pressure applied on the humeral head. Anterior Dislocation Management:
Stimson (Hanging Arm) : • * Best for elderly or obese pt. • *BUT : Slow, time consuming, fatiguing, unsuitable for tall patients, PainfulPosition. Anterior Dislocation Management:
Anterior Dislocation Spaso’s Method: “Reverse Stimson” Pt. supine position: grasp the affected arm at the wrist or forearm and lift gently vertically Traction, externally rotate . If still palpate and gently push the humeral head posteriorly with the opposite hand.
Anterior Dislocation Spaso’s Method “Reverse Stimson” Simple, effective, atraumatic. Safe reduction technique. Requiring minimal force and a single operator only.
Anterior Dislocation Chair Method: Pt. sit upright on a chair with a well-padded backrest. Using the backrest as fulcrum in the axilla gentle downward traction with external rotation is applied to the wrist.
Anterior Dislocation Self-reduction method: With 90° flexed ipsilateral knee pt. leans backward with neck in hyperextension, extending the elbows and hip. So Shoulder rotating the scapula around a vertical axis. Success = 60% ; SubCoracoid Less successful >60 years of age, subclavicular and especially subglenoid dislocations.