Download
1 / 32
380 likes | 563 Vues
ROLE OF COMPOSITE INDICES AND SYSTEMIC BIOMARKERS IN COPD. Prof. NIKOS SIAFAKAS MD,PhD,FRCP MEDICAL SCHOOL, UNIVERSITY OF CRETE, GREECE President of ERS 2009-2010. CONTENTS. Spirometry (FEV1) BODE index Biomarkers a) simple b) genetic.

E N D
ROLE OF COMPOSITE INDICES AND SYSTEMIC BIOMARKERS IN COPD Prof. NIKOS SIAFAKAS MD,PhD,FRCP MEDICAL SCHOOL, UNIVERSITY OF CRETE, GREECE President of ERS 2009-2010
CONTENTS Spirometry (FEV1) BODE index Biomarkers a) simple b) genetic
Patient-centered biomarkersBODE index Celli BR et al NEJM 2004
The BODE index, a simple multidimensional grading system, is better than the FEV1atpredicting the risk of death from any cause and from respiratory causes among patientswith COPD. Celli BR et al NEJM 2004
BODE index canbe used to determine the magnitude of the effect ofexacerbations on patients with COPD. The frequency of exacerbations negativelyimpacted on the progression of disease severityas measured by the BODE index. Chest 2007
The BODE index helps to stratify disease severity and its changes related to the progression of disease.
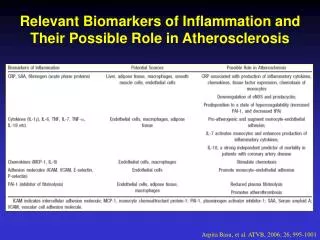
How a Biomarker is defined? • The use of biomarkers in medicine lies in their ability to detect disease and support diagnostic and therapeutic decisions. • As Biomarker, is defined any biochemical feature, or molecule, or material (cells, tissue), that can be measured in the body or its products, and which could reflect the disease process or predict its outcome. • A suitable biomarker should be reproducible, sensitive, specific, easy and cheap to determine, and should present a high predictive value. Barnes PJ et al AJRCCM 2006
Biomarkers in COPD • Several attempts to identify biomarker(s) have been made that are related to disease pathophysiology, the inflammatory and destructive processes . • However, there are still significant questions: -How the above biomarkers relate to COPD severity? -How reproducible they are? -How they may be affected by concurrent therapies? -How they relate to other disease measurements, such as FEV1 decline, exacerbation frequency, and mortality.
In INDUCED SPUTUM • Sputum induction is a practical and safe procedure and an important research tool of local inflammation in the lung. • Repeatability of induced sputum cellular counts and inflammatory mediators is satisfactory, even over extended periods of time and normal ranges derived from a relatively large adult population have been published. • Induced sputum is sampled predominantly from large airways, thus, may not reflect the peripheral inflammation that may be important in COPD outcome. Barnes PJ et al AJRCCM 2006, Chung KF ERJ 2001, Beeh KM et al CHEST 2003, Nightingale J et al Thorax 1998.
Biomarkers of COPD in induced sputum Tzortzaki E, et al. Curr Med. Chem 2007
In EXHALED AIR CONDENSATE • Exhaled breath condensate (EBC) is a non-invasive method for obtaining samples from the lung. • EBC contains several volatile chemicals (nitric oxide, carbon monoxide, hydrocarbons) and many non-volatile molecules (mediators, oxidation nitration products, peptides and cytokines), which have been used to quantify inflammation and oxidative stress in the respiratory trac • However, there are significant methodological considerations related to variability in the degree of dilution, which does not allow precise assessment of individual solute concentrations within native airway lining fluid. Barnes, P.J. Pharmacol. Rev., 2004 Horvath Iet al ERJ 2005.
Biomarkers of COPD, in exhaled air condensate Tzortzaki E, et al. Curr Med. Chem 2007
In PERIPHERAL BLOOD • Circulating neutrophils from COPD patients show enhanced respiratory burst compared with smokers with normal lung function. • Peripheral blood mononuclear cells from COPD patients demonstrate increased chemotactic responses compared to healthy smokers and receptor studies using flow cytometry have shown that monocyte expression of CXCR2 is regulated differently in COPD patients than in healthy smokers. • Monocyte TGF-beta production has been also found increased Circulating T-lymphocytes from COPD patients demonstrate increased apoptosis, along with up-regulation of the apoptotic pathways, TGF-beta, TNF-a and Fas. • Peripheral blood T-lymphocyte abnormalities might be different depending on the disease phenotype, as increased CD8+ve cell numbers and decreased CD4/CD8 ratios have been associated with small airway disease. Traves SL, et al. J Leukoc Biol, 2004 Kim WDet al. Chest, 2002 Hodge SJ et al. Am J Physiol Lung Cell Mol Physiol, 2003
Biomarkers of COPD, in peripheral blood Tzortzaki E, et al. Curr Med. Chem 2007
In URINE • Urine sample analysis is an easy method to measure elastin breakdown and collagen degradation products (urinary desmosine: a marker of mature elastin degradation,) • Markers of oxidative stress, like 8-hydroxydeoxyguanosine Also, 8- Isoprostane, a lipid peroxidation product was increased. • Thromboxane levels were increased in urine samples of COPD patients, compared to controls and correlated with the degree of hypoxia. • Issues to be considered: -methodological differences between laboratories, -minimum number of manipulations would avoid indeterminate losses of analytes, -urine markers respond to variations in the clinical conditions of the subjects. Annovazi et al, Electrophoresis 2004
Biomarkers of COPD, in urine Tzortzaki E, et al. Curr Med. Chem 2007
In BAL & BRONCHIAL BIOPSIES Bronchoscopic biopsy provides airway wall tissue from which the morphology can be assessed, inflammatory cells can be quantified, and gene products identified. Such studies increase our understanding of the disease process in COPD, and can contribute to the development of new treatments. Hattotuwa K et al. Chest, 2002
Overview of Biomarkers of COPD, in bronchial biopsies and BALF.
Pathway and candidate genes, by chromosomal region associated with COPD. Sampsonas F. et al. Curr. Med. Chem 2006; Tzortzaki et al, CCA 2006; Hersch et al, AJRCMB 2005
COPD & Markers of GENETIC INSTABILITY
THE PROPOSED MODEL FOR THE INITIATION OF COPD Oxidative stress Oxidative DNA damage of LEBCs Inactivation of DNA mismatch repair Somatic mutations of LEBCs Aberrant Host Immune Response Towards “damaged” LEBCs Cell Death Cascades Figure 1.
MSI COPD (59) 23% Healthy (60) 0%
COPD vs Asthma : MSI p<0.001 49.2 % positive MSI 22.2 COPD ASTHMA % positive MSI Mild Moderate Severe Very Severe Zervou et al, ERJ 2006 COPD ASTHMA
MSI & COPD EXACERBATIONS: Conclusions • The annual rate of severe exacerbations was greater for those exhibited MSI (p=0.02). • The rate was significantly greater in those subjects exhibited MSI in perforin related G29802 marker [p=0.03]. Makris et al, ERJ 2008
Conclusions • COPD lacks established and viable biomarkers to monitor disease progression, severity, clinical subtypes, or response to therapy. • Many candidate biomarkers were evaluated revealing a high degree of redundancy. • A recent meta-analysis of over 652 published studies, including 146.255 COPD patients, suggested that few of these biomarkers have been validated, and there is little information about reproducibility and the relationship to disease development, severity, or progression (Luigi G et al. Pulm Pharm Therap 2006)
Molecular Pulmonology Research Laboratory Prof. N. M. Siafakas E. Tzortzaki N. Tzanakis E. Vlachaki M. Siganaki M. Tsoumakidou M. Paraskakis M. Zervou K. Samara A. Karatzanis D. Makris University Hospital, Heraklion Crete