Download
1 / 7
80 likes | 287 Vues
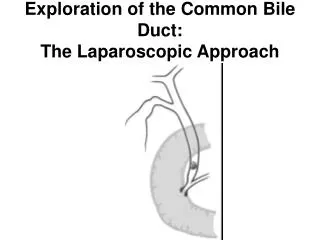
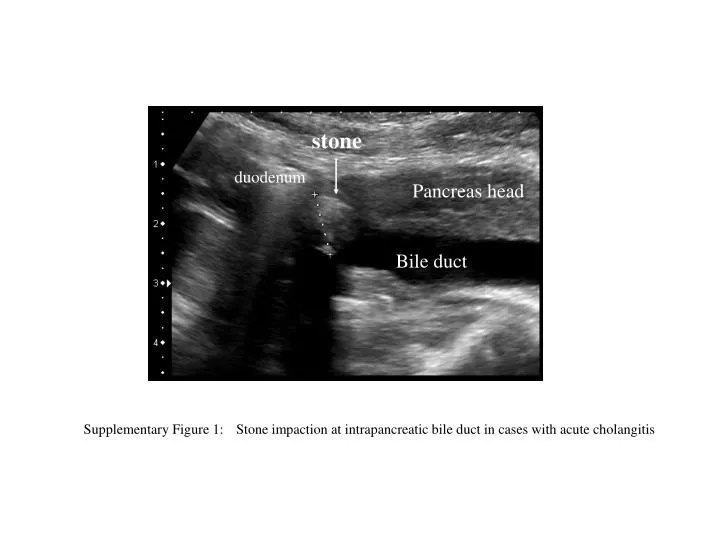
stone. duodenum. Pancreas head. Bile duct. Supplementary Figure 1: Stone impaction at intrapancreatic bile duct in cases with acute cholangitis. liver. tumor. Bile duct. Supplementary Figure 2: Cholangioma complicated with acute cholangitis.

E N D
stone duodenum Pancreas head Bile duct Supplementary Figure 1: Stone impaction at intrapancreatic bile duct in cases with acute cholangitis
liver tumor Bile duct Supplementary Figure 2:Cholangioma complicated with acute cholangitis Marked intrahepatic bile duct dilatation due to the obstruction by cholangioma is demonstrated.
A C E B D F Supplementary Figure 3: Acute cholangitis with gallstone and papillary tumor of the duodenum (77 years old female) A, B. precontrast CT,C, D. arterial phase of dynamic CT,E, F. equilibrium phase Precontrast CT shows gallstone (B: arrow).Arterial phase of dynamic CT shows enhanced papillary tumor of the duodenum (D: arrowhead). The liver parenchyma show inhomogeneous enhancement surrounding bile ducts indicating acute cholangitis. On equilibrium phase, inhomogeneous enhancement disappears.
A. on admission B. after EST therapy Supplementary Figure 4: Acute cholangitis with common bile duct stone, pre and post EST therapy Arterial phase of dynamic CT on admission (A) shows dilatation of intrahepatic bile ducts and inhomogeneous enhancement. After the removal of commonbile duct stone by EST, inhomogeneous enhancement disappears on follow up dynamic CT (B).
B A C D Supplementary Figure 5: Acute cholecystitis and cholangitis due to non-calcified gallstones (54 year old male) Contrast enhanced CT (A,B) show gallbladder distention with wall thickening. Gallstones are not detected on CT. Ultrasonography (C) shows two gallstones (arrowhead) with impaction with gallbladder neck. MRCP (D) also depicts two gallstones (arrowhead) clearly.
* * A B C Supplementary Figure 6: Hepatic abscess undergoing antibiotic therapy (64 year old male) Arterial phase of dynamic CT (A) shows double-target sign (arrow) and segmental enhancement (arrowhead). Equilibrium phase of dynamic CT (B) shows central hypodense abscess cavity (*) with peripheral enhancement (arrow). Segmental enhancement disappear. Follow-up arterial phase of dynamic CT (D)10 days after antibiotics therapy shows decrease in segmental enhancement (arrowhead) and size of abscess cavity. CT images are cited from a paper below Gabata T, Kodoya M, Matsui O, et al. Dynamic CT of Hepatic Abscesses: Significance of Transient Segmental Enhancement. AJR 2001;176:675-679
B A Supplementary Figure 7: Obstructive jaundice with cholangitis (74 year old male) MRCP (A) and coronal T2-weighted MR images clearly depict marked intrahepatic bile duct dilatation due to biliary obstruction by hepatic hilar tumor (arrowhead). Distal common bile duct also become dilated caused stone impaction (arrow).